Контроль рождаемости , также известный как контрацепция , антиконцепция и контроль фертильности , представляет собой использование методов или устройств для предотвращения нежелательной беременности . [1] Контроль рождаемости использовался с древних времен, но эффективные и безопасные методы контроля рождаемости стали доступны только в 20 веке. [2] Планирование, предоставление и использование контроля рождаемости человеком называется планированием семьи . [3] [4] Некоторые культуры ограничивают или препятствуют доступу к контролю рождаемости, поскольку считают его нежелательным с моральной, религиозной или политической точки зрения. [2]
У подростков беременность подвержена большему риску неблагоприятных исходов. [14] Всестороннее половое воспитание и доступ к средствам контроля рождаемости снижают частоту непреднамеренных беременностей в этой возрастной группе. [14] [15] Хотя все формы контроля рождаемости, как правило, могут использоваться молодыми людьми, [16] длительно действующие обратимые средства контроля рождаемости , такие как имплантаты, ВМС или вагинальные кольца, более успешны в снижении частоты подростковой беременности. [15] После родов женщина, которая не кормит исключительно грудью, может снова забеременеть всего через четыре-шесть недель. [16] Некоторые методы контроля рождаемости можно начинать сразу после родов, в то время как другие требуют задержки до шести месяцев. [16] У женщин, кормящих грудью, методы, содержащие только прогестин, предпочтительнее комбинированных оральных противозачаточных таблеток . [16] Женщинам, достигшим менопаузы , рекомендуется продолжать контроль рождаемости в течение одного года после последней менструации . [16]
Около 222 миллионов женщин, которые хотят избежать беременности в развивающихся странах , не используют современные методы контроля рождаемости. [17] [18] Использование контроля рождаемости в развивающихся странах снизило количество смертей во время или около беременности на 40% (около 270 000 смертей предотвращено в 2008 году) и могло бы предотвратить 70%, если бы был удовлетворен полный спрос на контроль рождаемости. [19] [20] Увеличивая время между беременностями, контроль рождаемости может улучшить результаты родов у взрослых женщин и выживание их детей. [19] В развивающихся странах доходы женщин, активы и вес, а также образование и здоровье их детей улучшаются с большим доступом к контролю рождаемости. [21] Контроль рождаемости увеличивает экономический рост из-за меньшего количества детей-иждивенцев, большего количества женщин, участвующих в рабочей силе , и/или меньшего использования ограниченных ресурсов. [21] [22]
Видео, объясняющее, как предотвратить нежелательную беременность
Методы
Методы контроля рождаемости включают барьерные методы , гормональный контроль рождаемости , внутриматочные спирали (ВМС), стерилизацию и поведенческие методы. Они используются до или во время секса, в то время как экстренные контрацептивы эффективны в течение пяти дней после секса. Эффективность обычно выражается как процент женщин, которые забеременели, используя данный метод в течение первого года, [27] а иногда как пожизненный показатель неудач среди методов с высокой эффективностью, таких как перевязка маточных труб . [28]
Наиболее эффективными являются методы длительного действия, не требующие постоянных визитов к врачу. [29] Хирургическая стерилизация, имплантируемые гормоны и внутриматочные спирали имеют показатели неудач в первый год менее 1%. [23] Гормональные контрацептивы, пластыри или вагинальные кольца, а также метод лактационной аменореи (LAM), если строго соблюдать их, также могут иметь показатели неудач в первый год (или для LAM первые 6 месяцев) менее 1%. [29] При типичном использовании показатели неудач в первый год значительно выше, на 9%, из-за непоследовательного использования. [23] Другие методы, такие как презервативы, диафрагмы и спермициды, имеют более высокие показатели неудач в первый год даже при идеальном использовании. [29] Американская академия педиатрии рекомендует обратимые противозачаточные средства длительного действия в качестве первой линии для молодых людей. [30]
Хотя все методы контроля рождаемости имеют некоторые потенциальные побочные эффекты, риск меньше, чем риск беременности. [29] После прекращения или удаления многих методов контроля рождаемости, включая оральные контрацептивы, ВМС, имплантаты и инъекции, уровень беременности в течение последующего года такой же, как и у тех, кто не использовал никаких методов контроля рождаемости. [31]
Для людей с определенными проблемами со здоровьем некоторые формы контроля рождаемости могут потребовать дополнительных исследований. [32] Для женщин, которые в остальном здоровы, многие методы контроля рождаемости не должны требовать медицинского обследования , включая противозачаточные таблетки, инъекционные или имплантируемые противозачаточные средства и презервативы. [33] Например, гинекологический осмотр , осмотр груди или анализ крови перед началом приема противозачаточных таблеток, по-видимому, не влияют на результаты. [34] [35] [36] В 2009 году Всемирная организация здравоохранения (ВОЗ) опубликовала подробный список медицинских критериев приемлемости для каждого типа контроля рождаемости. [32]
Гормональный
Гормональная контрацепция доступна в различных формах, включая оральные таблетки , имплантаты под кожу, инъекции , пластыри , ВМС и вагинальное кольцо . В настоящее время они доступны только для женщин, хотя гормональные контрацептивы для мужчин прошли и проходят клинические испытания. [37] Существует два типа оральных противозачаточных таблеток: комбинированные оральные контрацептивные таблетки (содержащие как эстроген , так и прогестин ) и таблетки, содержащие только прогестин (иногда называемые мини-пилюлями). [38] Если любой из них принимается во время беременности, они не увеличивают риск выкидыша и не вызывают врожденных дефектов . [35] Оба типа противозачаточных таблеток предотвращают оплодотворение, в основном, путем подавления овуляции и сгущения цервикальной слизи. [39] [40] Они также могут изменять слизистую оболочку матки и, таким образом, уменьшать имплантацию. [40] Их эффективность зависит от соблюдения пользователем режима приема таблеток. [35]
Комбинированные гормональные контрацептивы связаны с несколько повышенным риском образования венозных и артериальных тромбов . [41] Венозные тромбы, в среднем, увеличиваются с 2,8 до 9,8 на 10 000 женщин в год [42], что все еще меньше, чем связано с беременностью. [41] Из-за этого риска они не рекомендуются женщинам старше 35 лет, которые продолжают курить. [43] Из-за повышенного риска они включены в инструменты принятия решений, такие как оценка DASH и правило PERC, используемые для прогнозирования риска образования тромбов. [44]
Влияние на половое влечение различно, с увеличением или уменьшением в некоторых случаях, но без эффекта в большинстве случаев. [45] Комбинированные оральные контрацептивы снижают риск рака яичников и рака эндометрия и не изменяют риск рака молочной железы. [46] [47] Они часто уменьшают менструальное кровотечение и болезненные менструальные спазмы . [35] Более низкие дозы эстрогена, высвобождаемые из вагинального кольца, могут снизить риск болезненности груди, тошноты и головной боли, связанных с более высокими дозами эстрогеновых продуктов. [46]
Таблетки, инъекции и внутриматочные спирали, содержащие только прогестин, не связаны с повышенным риском образования тромбов и могут использоваться женщинами с историей образования тромбов в венах. [41] [48] Тем, у кого в анамнезе были артериальные тромбы, следует использовать негормональные противозачаточные средства или метод, содержащий только прогестин, отличный от инъекционной версии. [41] Таблетки, содержащие только прогестин, могут улучшить менструальные симптомы и могут использоваться кормящими женщинами, поскольку они не влияют на выработку молока . Нерегулярные кровотечения могут возникать при использовании методов, содержащих только прогестин, при этом некоторые пользователи сообщают об отсутствии менструаций . [49] Прогестины дроспиренон и дезогестрел минимизируют андрогенные побочные эффекты, но увеличивают риск образования тромбов и, таким образом, не являются препаратами первой линии. [50] Идеальный показатель неудач в первый год использования инъекционного прогестина составляет 0,2%; типичный показатель неудач в первый год использования составляет 6%. [23]
Во всем мире презервативы являются наиболее распространенным методом контроля рождаемости. [52] Мужские презервативы надеваются на эрегированный половой член мужчины и физически блокируют попадание эякулированной спермы в тело полового партнера. [53] Современные презервативы чаще всего изготавливаются из латекса , но некоторые из них изготавливаются из других материалов, таких как полиуретан или кишки ягненка. [53] Также доступны женские презервативы , чаще всего изготавливаемые из нитрила , латекса или полиуретана. [54] Мужские презервативы имеют то преимущество, что они недорогие, простые в использовании и имеют мало побочных эффектов. [55] Обеспечение доступности презервативов для подростков, по-видимому, не влияет на возраст начала половой жизни или ее частоту. [56] В Японии около 80% пар, использующих противозачаточные средства, используют презервативы, в то время как в Германии этот показатель составляет около 25%, [57] а в Соединенных Штатах — 18%. [58]
Мужские презервативы и диафрагма со спермицидом имеют типичные показатели отказа в первый год использования 18% и 12% соответственно. [23] При идеальном использовании презервативы более эффективны с показателем отказа в первый год 2% по сравнению с показателем в первый год 6% с диафрагмой. [23] Презервативы имеют дополнительное преимущество, помогая предотвратить распространение некоторых инфекций, передающихся половым путем, таких как ВИЧ/СПИД , однако презервативы, изготовленные из кишечника животных, этого не делают. [7] [59]
Контрацептивные губки сочетают в себе барьер со спермицидом. [29] Как и диафрагмы, они вводятся вагинально перед половым актом и должны быть помещены на шейку матки, чтобы быть эффективными. [29] Типичные показатели неудач в течение первого года зависят от того, рожала ли женщина ранее, составляя 24% у тех, у кого были роды, и 12% у тех, у кого их не было. [23] Губку можно вводить за 24 часа до полового акта и ее необходимо оставлять на месте в течение как минимум шести часов после него. [29] Сообщалось об аллергических реакциях [60] и более серьезных побочных эффектах, таких как синдром токсического шока . [61]
Современные внутриматочные средства (ВМС) представляют собой небольшие устройства, часто Т-образной формы, содержащие либо медь, либо левоноргестрел , которые вводятся в матку. Они являются одной из форм длительно действующей обратимой контрацепции , которая является наиболее эффективным типом обратимого контроля рождаемости. [62] Частота неудач при использовании медной ВМС составляет около 0,8%, в то время как частота неудач при использовании левоноргестреловой ВМС составляет 0,2% в течение первого года использования. [63] Среди типов контроля рождаемости они, наряду с противозачаточными имплантатами, вызывают наибольшее удовлетворение у пользователей. [64] По состоянию на 2007 год [update]ВМС являются наиболее широко используемой формой обратимой контрацепции, с более чем 180 миллионами пользователей по всему миру. [65]
Доказательства подтверждают эффективность и безопасность для подростков [64] и тех, у кого есть и не было детей. [66] ВМС не влияют на грудное вскармливание и могут быть введены сразу после родов. [67] Их также можно использовать сразу после аборта. [68] [69] После удаления, даже после длительного использования, фертильность немедленно возвращается к норме. [70]
В то время как медные ВМС могут усиливать менструальное кровотечение и приводить к более болезненным спазмам, [71] гормональные ВМС могут уменьшать менструальное кровотечение или полностью прекращать менструацию. [67] Спазмы можно лечить с помощью обезболивающих, таких как нестероидные противовоспалительные препараты . [72] Другие потенциальные осложнения включают изгнание (2–5%) и редко перфорацию матки (менее 0,7%). [67] [72] Предыдущая модель внутриматочной спирали ( щит Dalkon ) была связана с повышенным риском воспалительных заболеваний органов малого таза ; однако, риск не влияет на риск при использовании современных моделей у тех, у кого не было инфекций, передающихся половым путем , во время введения. [73] ВМС, по-видимому, снижают риск рака яичников . [74]
Стерилизация
Существуют две основные категории: хирургические и нехирургические.
Хирургическая стерилизация доступна в форме перевязки маточных труб для женщин и вазэктомии для мужчин. [2] Перевязка маточных труб снижает риск рака яичников . [2] Краткосрочные осложнения в двадцать раз менее вероятны при вазэктомии, чем при перевязке маточных труб. [2] [75] После вазэктомии может возникнуть отек и боль в мошонке, которые обычно проходят через одну или две недели. [76] Хроническая боль в мошонке, связанная с негативным влиянием на качество жизни, возникает после вазэктомии примерно у 1–2% мужчин. [77] При перевязке маточных труб осложнения возникают в 1–2 процентах случаев, причем серьезные осложнения обычно связаны с анестезией . [78] Ни один из методов не обеспечивает защиты от инфекций, передающихся половым путем. [2] Иногда сальпингэктомию также используют для стерилизации у женщин. [79]
Также были изучены нехирургические методы стерилизации . Фахим [80] [81] [82] и др. обнаружили, что тепловое воздействие, особенно ультразвук высокой интенсивности, было эффективным как для временной, так и для постоянной контрацепции в зависимости от дозы, например, селективное разрушение половых клеток и клеток Сертоли без воздействия на клетки Лейдига или уровень тестостерона. Также доступны химические, например, лекарственные методы, например, пероральный прием лонидамина [83] для временного или постоянного (в зависимости от дозы) управления фертильностью. Борис [84] предлагает метод химической индукции либо временной, либо необратимой стерильности в зависимости от дозы: «Постоянная стерильность у мужчин может быть получена с помощью однократной пероральной дозы, содержащей от около 18 мг/кг до около 25 мг/кг».
Постоянство этого решения может вызвать сожаление у некоторых мужчин и женщин. Из женщин, перенесших перевязку маточных труб после 30 лет, около 6% сожалеют о своем решении, по сравнению с 20–24% женщин, прошедших стерилизацию в течение года после родов и до достижения 30 лет, и 6% среди нерожавших женщин, стерилизованных до 30 лет . [85] Напротив, менее 5% мужчин, вероятно, пожалеют о стерилизации. Мужчины, которые с большей вероятностью пожалеют о стерилизации, моложе, имеют маленьких детей или не имеют их вообще, или находятся в нестабильном браке. [86] В опросе биологических родителей 9% заявили, что не имели бы детей, если бы могли сделать это снова. [87]
Хотя стерилизация считается постоянной процедурой, [88] можно попытаться провести трубную реверсию , чтобы снова соединить фаллопиевы трубы , или вазэктомию, чтобы снова соединить семявыносящие протоки . У женщин желание реверсии часто связано со сменой супруга. [88] Показатели успешной беременности после трубной реверсии составляют от 31 до 88 процентов, с осложнениями, включая повышенный риск внематочной беременности . [88] Число мужчин, которые просят реверсию, составляет от 2 до 6 процентов. [89] Показатели успешного отцовства еще одного ребенка после реверсии составляют от 38 до 84 процентов; при этом успех тем ниже, чем дольше период времени между вазэктомией и реверсией. [89] Извлечение спермы с последующим экстракорпоральным оплодотворением также может быть вариантом для мужчин. [90]
Поведенческий
Поведенческие методы включают регулирование времени или способа полового акта для предотвращения попадания спермы в женские половые пути, либо вообще, либо когда может присутствовать яйцеклетка. [91] При идеальном использовании уровень неудач в первый год может составлять около 3,4%; однако при неправильном использовании уровень неудач в первый год может приближаться к 85%. [92]
Осведомленность о фертильности
Инструмент CycleBeads , используемый для оценки фертильности на основе количества дней с момента последней менструации.
Методы определения фертильности включают определение наиболее фертильных дней менструального цикла и избегание незащищенного полового акта. [91] Методы определения фертильности включают мониторинг базальной температуры тела , цервикальных выделений или дня цикла. [91] Они имеют типичные показатели неудач в первый год 24%; идеальное использование показателей неудач в первый год зависит от того, какой метод используется, и варьируется от 0,4% до 5%. [23] Однако доказательства, на которых основаны эти оценки, недостаточны, поскольку большинство людей в испытаниях прекращают их использование рано. [91] Во всем мире их используют около 3,6% пар. [93] Если основываться как на базальной температуре тела, так и на другом первичном признаке, метод называется симптотермальным. В клинических исследованиях симптотермального метода сообщалось о показателях неудач в первый год 20% в целом и 0,4% при идеальном использовании. [94] [23] По состоянию на 2016 год доступно несколько приложений для отслеживания фертильности , но они, как правило, предназначены для помощи тем, кто пытается забеременеть, а не для предотвращения беременности. [95]
Снятие
Метод прерывания полового акта (также известный как прерванный половой акт) — это практика прекращения полового акта («вытаскивание») до эякуляции. [96] Основной риск метода прерывания полового акта заключается в том, что мужчина может выполнить маневр неправильно или несвоевременно. [96] Показатели неудач в течение первого года варьируются от 4% при идеальном использовании до 22% при типичном использовании. [23] Некоторые медицинские специалисты не считают его средством контроля рождаемости. [29]
Существует мало данных относительно содержания спермы в предэякуляторной жидкости . [97] Хотя некоторые предварительные исследования не обнаружили сперму, [97] одно исследование обнаружило наличие спермы у 10 из 27 добровольцев. [98] Метод прерывания полового акта используется в качестве контроля рождаемости примерно 3% пар. [93]
Воздержание
Половое воздержание может использоваться как форма контроля рождаемости, что означает либо не заниматься никакой сексуальной активностью, либо конкретно не заниматься вагинальным сексом, занимаясь другими формами невагинального секса. [99] [100] Полное половое воздержание на 100% эффективно для предотвращения беременности. [101] [102] Однако среди тех, кто дает обещание воздерживаться от добрачного секса , до 88% тех, кто занимается сексом, делают это до брака. [103] Выбор воздерживаться от секса не может защитить от беременности в результате изнасилования, и усилия общественного здравоохранения, подчеркивающие воздержание для сокращения нежелательной беременности, могут иметь ограниченную эффективность, особенно в развивающихся странах и среди неблагополучных групп . [104] [105]
Преднамеренный непроникающий секс без вагинального секса или преднамеренный оральный секс без вагинального секса также иногда считаются контролем рождаемости. [99] Хотя это, как правило, позволяет избежать беременности, беременность все еще может наступить при межножковом сексе и других формах секса с половым членом около влагалища (трение гениталий и выход полового члена из анального секса ), когда сперма может быть отложена около входа во влагалище и может перемещаться по смазочным жидкостям влагалища. [106] [107]
Половое воспитание, основанное только на воздержании, не снижает подростковую беременность . [9] [108] Показатели подростковой беременности и показатели ИППП, как правило, одинаковы или выше в штатах, где учащимся предоставляется образование, основанное только на воздержании, по сравнению с комплексным половым воспитанием . [108] Некоторые органы власти рекомендуют тем, кто использует воздержание в качестве основного метода, иметь под рукой резервные методы (например, презервативы или таблетки экстренной контрацепции). [109]
Лактация
Метод лактационной аменореи подразумевает использование естественного послеродового бесплодия женщины , которое возникает после родов и может быть продлено грудным вскармливанием . [110] Для того, чтобы послеродовая женщина была бесплодной (защищенной от беременности), ее месячные, как правило, еще не восстановились (не было менструаций), она кормит ребенка исключительно грудью, и ребенку меньше шести месяцев. [26] Если грудное вскармливание является единственным источником питания ребенка, а ребенку меньше 6 месяцев, то, по оценкам, 93–99% женщин защищены от беременности в первые шесть месяцев (показатель неудач 0,75–7,5%). [111] [112] Показатель неудач увеличивается до 4–7% в течение одного года и 13% в течение двух лет. [113] Кормление смесью, сцеживание вместо кормления грудью, использование соски-пустышки и кормление твердой пищей увеличивают шансы забеременеть во время грудного вскармливания. [114] У тех, кто кормит исключительно грудью, примерно у 10% менструации начинаются до трех месяцев, а у 20% — до шести месяцев. [113] У тех, кто не кормит грудью, фертильность может восстановиться уже через четыре недели после родов. [113]
Экстренные методы контрацепции — это лекарства (иногда ошибочно называемые «таблетками на следующее утро») [115] или устройства, используемые после незащищенного полового акта в надежде предотвратить беременность. Экстренные контрацептивы часто даются жертвам изнасилования. [10] Они работают в основном путем предотвращения овуляции или оплодотворения. [2] [116] Они вряд ли повлияют на имплантацию, но это не было полностью исключено. [116] Существует ряд вариантов, включая высокодозированные противозачаточные таблетки , левоноргестрел , мифепристон , улипристал и ВМС. [117] Все методы имеют минимальные побочные эффекты. [117] Предоставление экстренных противозачаточных таблеток женщинам до начала половой жизни не влияет на показатели инфекций, передающихся половым путем, использование презервативов, показатели беременности или рискованное сексуальное поведение. [118] [119] В исследовании, проведенном в Великобритании, когда фармацевт предоставил трехмесячный «мостовой» запас таблеток, содержащих только прогестоген, вместе с экстренной контрацепцией после сексуальной активности, было показано, что это вмешательство увеличивает вероятность того, что человек начнет использовать эффективный метод долгосрочной контрацепции. [120] [121]
Таблетки левоноргестрела при использовании в течение 3 дней снижают вероятность беременности после одного эпизода незащищенного секса или отказа презерватива на 70% (что приводит к частоте наступления беременности 2,2%). [10] Улипристал при использовании в течение 5 дней снижает вероятность беременности примерно на 85% (частота наступления беременности 1,4%) и более эффективен, чем левоноргестрел. [10] [117] [122] Мифепристон также более эффективен, чем левоноргестрел, в то время как медные ВМС являются наиболее эффективным методом. [117] ВМС можно вводить в течение пяти дней после полового акта, и они предотвращают около 99% беременностей после эпизода незащищенного секса (частота наступления беременности от 0,1 до 0,2%). [2] [123] Это делает их наиболее эффективной формой экстренной контрацепции. [124] У людей с избыточным весом или ожирением левоноргестрел менее эффективен, и рекомендуется использовать ВМС или улипристал. [125]
Двойная защита
Двойная защита — это использование методов, которые предотвращают как инфекции, передающиеся половым путем , так и беременность. [126] Это может быть как использование презервативов в отдельности, так и совместно с другим методом контроля рождаемости или избегание проникающего секса . [127] [128]
Если беременность вызывает серьезные опасения, разумно использовать два метода одновременно. [127] Например, две формы контроля рождаемости рекомендуются тем, кто принимает препарат от угревой сыпи изотретиноин или противоэпилептические препараты , такие как карбамазепин , из-за высокого риска врожденных дефектов при приеме во время беременности. [129] [130]
Эффекты
Здоровье
Уровень материнской смертности по состоянию на 2010 год. [131]Использование средств контроля рождаемости и общий коэффициент рождаемости по регионам.
Использование контрацептивов в развивающихся странах , по оценкам, снизило количество материнских смертей на 40% (около 270 000 смертей предотвращено в 2008 году) и могло бы предотвратить 70% смертей, если бы был удовлетворен полный спрос на контроль рождаемости. [19] [20] Эти преимущества достигаются за счет сокращения количества незапланированных беременностей, которые впоследствии приводят к небезопасным абортам, и за счет предотвращения беременностей у тех, кто находится в группе высокого риска. [19]
Контроль рождаемости также повышает выживаемость детей в развивающихся странах за счет увеличения промежутков между беременностями. [19] В этой группе населения результаты хуже, когда мать беременеет в течение восемнадцати месяцев после предыдущих родов. [19] [132] Однако отсрочка следующей беременности после выкидыша , по-видимому, не снижает риск, и женщинам рекомендуется попытаться забеременеть в этой ситуации, когда они будут готовы. [132]
Подростковая беременность , особенно среди молодых подростков, подвержена большему риску неблагоприятных исходов, включая ранние роды , низкий вес при рождении и смерть младенца . [14] В 2012 году в Соединенных Штатах 82% беременностей в возрасте от 15 до 19 лет были незапланированными. [72] Всестороннее половое воспитание и доступ к средствам контроля рождаемости эффективны для снижения показателей беременности в этой возрастной группе. [133]
Методы контроля рождаемости, особенно гормональные методы , также могут иметь нежелательные побочные эффекты. Интенсивность побочных эффектов может варьироваться от незначительных до изнурительных и зависит от индивидуального опыта. Чаще всего они включают изменение регулярности и потока менструаций, тошноту, болезненность груди, головные боли, увеличение веса и изменения настроения (в частности, усиление депрессии и тревожности). [134] [135] Кроме того, гормональная контрацепция может способствовать потере минеральной плотности костей, нарушению метаболизма глюкозы, повышению риска венозной тромбоэмболии. [135] [134] Всестороннее половое воспитание и прозрачное обсуждение побочных эффектов и противопоказаний к контролю рождаемости между поставщиком медицинских услуг и пациентом являются обязательными. [134]
Финансы
Карта стран по уровню рождаемости (2020)
В развивающихся странах контроль рождаемости увеличивает экономический рост из-за меньшего количества детей-иждивенцев и, таким образом, большего количества женщин, участвующих или увеличивающих вклад в рабочую силу , поскольку они обычно являются основными опекунами детей. [21] Заработки женщин, активы, индекс массы тела , а также обучение и индекс массы тела их детей улучшаются с большим доступом к контролю рождаемости. [21] Планирование семьи с помощью использования современных методов контроля рождаемости является одним из наиболее экономически эффективных вмешательств в здравоохранение. [136] По оценкам Организации Объединенных Наций, на каждый потраченный доллар экономится от двух до шести долларов. [18] Эта экономия средств связана с предотвращением незапланированной беременности и уменьшением распространения заболеваний, передающихся половым путем. [136] Хотя все методы выгодны в финансовом отношении, использование медных ВМС привело к наибольшей экономии. [136]
Общая стоимость медицинских услуг по беременности, родам и уходу за новорожденным в Соединенных Штатах в среднем составляет 21 000 долларов США за естественные роды и 31 000 долларов США за кесарево сечение по состоянию на 2012 год. [137] В большинстве других стран эта стоимость составляет менее половины. [137] На ребенка, родившегося в 2011 году, средняя американская семья потратит 235 000 долларов США за 17 лет, чтобы его вырастить. [138]
Распространенность
Карта мира, раскрашенная в соответствии с современным использованием средств контроля рождаемости. Каждый уровень затенения представляет собой диапазон из шести процентных пунктов, с использованием, меньшим или равным:
Спрос на планирование семьи, удовлетворенный современными методами по состоянию на 2017 год. [139]
По состоянию на 2009 год в мире около 60% тех, кто состоит в браке и может иметь детей, используют средства контроля рождаемости. [140] Частота использования различных методов сильно различается в разных странах. [140] Наиболее распространенным методом в развитых странах являются презервативы и оральные контрацептивы, в то время как в Африке это оральные контрацептивы, а в Латинской Америке и Азии — стерилизация. [140] В развивающихся странах в целом 35% средств контроля рождаемости осуществляется посредством женской стерилизации, 30% — посредством ВМС, 12% — посредством оральных контрацептивов, 11% — посредством презервативов и 4% — посредством мужской стерилизации. [140]
Хотя в развитых странах они используются реже, чем в развивающихся странах, число женщин, использующих ВМС, по состоянию на 2007 год составило более 180 миллионов. [65] Около 3,6% женщин детородного возраста избегают секса в фертильном возрасте, а в районах Южной Америки этот метод используют до 20%. [141] По состоянию на 2005 год 12% пар используют мужскую форму контроля рождаемости (презервативы или вазэктомию), причем в развитых странах этот показатель выше. [142] Использование мужских форм контроля рождаемости снизилось в период с 1985 по 2009 год . [140] Использование контрацептивов среди женщин в странах Африки к югу от Сахары возросло с примерно 5% в 1991 году до примерно 30% в 2006 году. [143]
По состоянию на 2012 год 57% женщин детородного возраста хотят избежать беременности (867 из 1520 миллионов). [144] Однако около 222 миллионов женщин не смогли получить доступ к средствам контроля рождаемости, 53 миллиона из которых находились в странах Африки к югу от Сахары, а 97 миллионов — в Азии. [144] Это приводит к 54 миллионам незапланированных беременностей и почти 80 000 случаев материнской смертности в год. [140] Одной из причин того, что многие женщины не имеют средств контроля рождаемости, является то, что многие страны ограничивают доступ к ним по религиозным или политическим причинам, [2] а другим фактором является бедность. [145] Из-за ограничительных законов об абортах в странах Африки к югу от Сахары многие женщины обращаются к нелицензированным поставщикам услуг по абортам для незапланированной беременности , в результате чего около 2–4% ежегодно делают небезопасные аборты . [145]
История
Ранняя история
Древняя серебряная монета из Кирены с изображением стебля сильфия
The Egyptian Ebers Papyrus from 1550 BC and the Kahun Papyrus from 1850 BC have within them some of the earliest documented descriptions of birth control: the use of honey, acacia leaves and lint to be placed in the vagina to block sperm.[146][147]Silphium, a species of giant fennel native to north Africa, may have been used as birth control in ancient Greece and the ancient Near East.[148][149] Due to its desirability, by the first century AD, it had become so rare that it was worth more than its weight in silver and, by late antiquity, it was fully extinct.[148] Most methods of birth control used in antiquity were probably ineffective.[150]
The ancient Greek philosopher Aristotle (c. 384–322 BC) recommended applying cedar oil to the womb before intercourse, a method which was probably only effective on occasion.[150] A Hippocratic text On the Nature of Women recommended that a woman drink a copper salt dissolved in water, which it claimed would prevent pregnancy for a year.[150] This method was not only ineffective, but also dangerous, as the later medical writer Soranus of Ephesus (c. 98–138 AD) pointed out.[150] Soranus attempted to list reliable methods of birth control based on rational principles.[150] He rejected the use of superstition and amulets and instead prescribed mechanical methods such as vaginal plugs and pessaries using wool as a base covered in oils or other gummy substances.[150] Many of Soranus's methods were probably also ineffective.[150]
In medieval Europe, any effort to halt pregnancy was deemed immoral by the Catholic Church,[146] although it is believed that women of the time still used a number of birth control measures, such as coitus interruptus and inserting lily root and rue into the vagina.[151] Women in the Middle Ages were also encouraged to tie weasel testicles around their thighs during sex to prevent pregnancy.[152] The oldest condoms discovered to date were recovered in the ruins of Dudley Castle in England, and are dated back to 1640.[152] They were made of animal gut, and were most likely used to prevent the spread of sexually transmitted infections during the English Civil War.[152]Casanova, living in 18th-century Italy, described the use of a lambskin covering to prevent pregnancy; however, condoms only became widely available in the 20th century.[146]
Birth control movement
"And the villain still pursues her", a satirical Victorian era postcard
The birth control movement developed during the 19th and early 20th centuries.[153] The Malthusian League, based on the ideas of Thomas Malthus, was established in 1877 in the United Kingdom to educate the public about the importance of family planning and to advocate for getting rid of penalties for promoting birth control.[154] It was founded during the "Knowlton trial" of Annie Besant and Charles Bradlaugh, who were prosecuted for publishing on various methods of birth control.[155]
In the United States, Margaret Sanger and Otto Bobsein popularized the phrase "birth control" in 1914.[156][157] Sanger primarily advocated for birth control on the idea that it would prevent women from seeking unsafe abortions, but during her lifetime, she began to campaign for it on the grounds that it would reduce mental and physical defects.[158][159] She was mainly active in the United States but had gained an international reputation by the 1930s. At the time, under the Comstock Law, distribution of birth control information was illegal. She jumped bail in 1914 after her arrest for distributing birth control information and left the United States for the United Kingdom.[160] In the U.K., Sanger, influenced by Havelock Ellis, further developed her arguments for birth control. She believed women needed to enjoy sex without fearing a pregnancy. During her time abroad, Sanger also saw a more flexible diaphragm in a Dutch clinic, which she thought was a better form of contraceptive.[159] Once Sanger returned to the United States, she established a short-lived birth-control clinic with the help of her sister, Ethel Bryne, based in the Brownville section of Brooklyn, New York[161] in 1916. It was shut down after eleven days and resulted in her arrest.[162] The publicity surrounding the arrest, trial, and appeal sparked birth control activism across the United States.[163] Besides her sister, Sanger was helped in the movement by her first husband, William Sanger, who distributed copies of "Family Limitation." Sanger's second husband, James Noah H. Slee, would also later become involved in the movement, acting as its main funder.[159] Sanger also contributed to the funding of research into hormonal contraceptives in the 1950s.[164] She helped fund research John Rock, and biologist Gregory Pincus that resulted in the first hormonal contraceptive pill, later called Enovid.[165] The first human trials of the pill were done on patients in the Worcester State Psychiatric Hospital, after which clinical testing was done in Puerto Rico before Enovid was approved for use in the U.S.. The people participating in these trials were not fully informed on the medical implications of the pill, and often had minimal to no other family planning options.[166][167] The newly approved birth control method was not made available to the participants after the trials, and contraceptives are still not widely accessible in Puerto Rico.[165]
The increased use of birth control was seen by some as a form of social decay.[168] A decrease of fertility was seen as a negative. Throughout the Progressive Era (1890–1920), there was an increase of voluntary associations aiding the contraceptive movement.[168] These organizations failed to enlist more than 100,000 women because the use of birth control was often compared to eugenics;[168] however, there were women seeking a community with like-minded women. The ideology that surrounded birth control started to gain traction during the Progressive Era due to voluntary associations establishing community. Birth control was unlike the Victorian Era because women wanted to manage their sexuality. The use of birth control was another form of self-interest women clung to. This was seen as women began to gravitate towards strong figures, like the Gibson Girl.[169]
The first permanent birth-control clinic was established in Britain in 1921 by Marie Stopes working with the Malthusian League.[170] The clinic, run by midwives and supported by visiting doctors,[171] offered women's birth-control advice and taught them the use of a cervical cap. Her clinic made contraception acceptable during the 1920s by presenting it in scientific terms. In 1921, Sanger founded the American Birth Control League, which later became the Planned Parenthood Federation of America.[172] In 1924 the Society for the Provision of Birth Control Clinics was founded to campaign for municipal clinics; this led to the opening of a second clinic in Greengate, Salford in 1926.[173] Throughout the 1920s, Stopes and other feminist pioneers, including Dora Russell and Stella Browne, played a major role in breaking down taboos about sex. In April 1930 the Birth Control Conference assembled 700 delegates and was successful in bringing birth control and abortion into the political sphere – three months later, the Ministry of Health, in the United Kingdom, allowed local authorities to give birth-control advice in welfare centres.[174]
The National Birth Control Association was founded in Britain in 1931, and became the Family Planning Association eight years later. The Association amalgamated several British birth control-focused groups into 'a central organisation' for administering and overseeing birth control in Britain. The group incorporated the Birth Control Investigation Committee, a collective of physicians and scientists that was founded to investigate scientific and medical aspects of contraception with 'neutrality and impartiality'.[175] Subsequently, the Association effected a series of 'pure' and 'applied' product and safety standards that manufacturers must meet to ensure their contraceptives could be prescribed as part of the Association's standard two-part-technique combining 'a rubber appliance to protect the mouth of the womb' with a 'chemical preparation capable of destroying... sperm'.[176] Between 1931 and 1959, the Association founded and funded a series of tests to assess chemical efficacy and safety and rubber quality.[177] These tests became the basis for the Association's Approved List of contraceptives, which was launched in 1937, and went on to become an annual publication that the expanding network of FPA clinics relied upon as a means to 'establish facts [about contraceptives] and to publish these facts as a basis on which a sound public and scientific opinion can be built'.[178]
In 1936, the United States Court of Appeals for the Second Circuit ruled in United States v. One Package of Japanese Pessaries that medically prescribing contraception to save a person's life or well-being was not illegal under the Comstock Laws. Following this decision, the American Medical Association Committee on Contraception revoked its 1936 statement condemning birth control.[179] A national survey in 1937 showed 71 percent of the adult population supported the use of contraception.[180] By 1938, 374 birth control clinics were running in the United States despite their advertisement still being illegal.[181]First LadyEleanor Roosevelt publicly supported birth control and family planning.[182] The restrictions on birth control in the Comstock laws were effectively rendered null and void by Supreme Court decisions Griswold v. Connecticut (1965)[183] and Eisenstadt v. Baird (1972).[184] In 1966, President Lyndon B. Johnson started endorsing public funding for family planning services, and the Federal Government began subsidizing birth control services for low-income families.[185]The Affordable Care Act, passed into law on March 23, 2010, under President Barack Obama, requires all plans in the Health Insurance Marketplace to cover contraceptive methods. These include barrier methods, hormonal methods, implanted devices, emergency contraceptives, and sterilization procedures.[186]
Modern methods
In 1909, Richard Richter developed the first intrauterine device made from silkworm gut, which was further developed and marketed in Germany by Ernst Gräfenberg in the late 1920s.[187] In 1951, an Austrian-born American chemist, named Carl Djerassi at Syntex in Mexico City made the hormones in progesterone pills using Mexican yams (Dioscorea mexicana).[188] Djerassi had chemically created the pill but was not equipped to distribute it to patients. Meanwhile, Gregory Pincus and John Rock with help from the Planned Parenthood Federation of America developed the first birth control pills in the 1950s, such as mestranol/noretynodrel, which became publicly available in the 1960s through the Food and Drug Administration under the name Enovid.[172][189]Medical abortion became an alternative to surgical abortion with the availability of prostaglandin analogs in the 1970s and mifepristone in the 1980s.[190]
Society and culture
Legal positions
Human rights agreements require most governments to provide family planning and contraceptive information and services. These include the requirement to create a national plan for family planning services, remove laws that limit access to family planning, ensure that a wide variety of safe and effective birth control methods are available including emergency contraceptives, make sure there are appropriately trained healthcare providers and facilities at an affordable price, and create a process to review the programs implemented. If governments fail to do the above it may put them in breach of binding international treaty obligations.[191]
In the United States, the 1965 Supreme Court decision Griswold v. Connecticut overturned a state law prohibiting dissemination of contraception information based on a constitutional right to privacy for marital relationships. In 1972, Eisenstadt v. Baird extended this right to privacy to single people.[192]
In 2010, the United Nations launched the Every Woman Every Child movement to assess the progress toward meeting women's contraceptive needs. The initiative has set a goal of increasing the number of users of modern birth control by 120 million women in the world's 69 poorest countries by 2020. Additionally, they aim to eradicate discrimination against girls and young women who seek contraceptives.[193] The American Congress of Obstetricians and Gynecologists (ACOG) recommended in 2014 that oral birth control pills should be over the counter medications.[194]
Since at least the 1870s, American religious, medical, legislative, and legal commentators have debated contraception laws. Ana Garner and Angela Michel have found that in these discussions men often attach reproductive rights to moral and political matters, as part of an ongoing attempt to regulate human bodies. In press coverage between 1873 and 2013 they found a divide between institutional ideology and real-life experiences of women.[195]
Religious views
Religions vary widely in their views of the ethics of birth control.[196] The Roman Catholic Church re-affirmed its teachings in 1968 that only natural family planning is permissible,[197] although large numbers of Catholics in developed countries accept and use modern methods of birth control.[198][199][200] The Greek Orthodox Church admits a possible exception to its traditional teaching forbidding the use of artificial contraception, if used within marriage for certain purposes, including the spacing of births.[201] Among Protestants, there is a wide range of views from supporting none, such as in the Quiverfull movement, to allowing all methods of birth control.[202] Views in Judaism range from the stricter Orthodox sect, which prohibits all methods of birth control, to the more relaxed Reform sect, which allows most.[203]Hindus may use both natural and modern contraceptives.[204] A common Buddhist view is that preventing conception is acceptable, while intervening after conception has occurred is not.[205] In Islam, contraceptives are allowed if they do not threaten health, although their use is discouraged by some.[206]
There are a number of common misconceptions regarding sex and pregnancy.[208]Douching after sexual intercourse is not an effective form of birth control.[209] Additionally, it is associated with a number of health problems and thus is not recommended.[210] Women can become pregnant the first time they have sexual intercourse[211] and in any sexual position.[212] It is possible, although not very likely, to become pregnant during menstruation.[213] Contraceptive use, regardless of its duration and type, does not have a negative effect on the ability of women to conceive following termination of use and does not significantly delay fertility. Women who use oral contraceptives for a longer duration may have a slightly lower rate of pregnancy than do women using oral contraceptives for a shorter period of time, possibly due to fertility decreasing with age.[214]
Accessibility
Access to birth control may be affected by finances and the laws within a region or country.[215] In the United States African American, Hispanic, and young women are disproportionately affected by limited access to birth control, as a result of financial disparity.[216][217] For example, Hispanic and African American women often lack insurance coverage and are more often poor.[218] New immigrants in the United States are not offered preventive care such as birth control.[219]
In the United Kingdom contraception can be obtained free of charge via contraception clinics, sexual health or GUM (genitourinary medicine) clinics, via some GP surgeries, some young people's services and pharmacies.[220][221]
In September 2021, France announced that women aged under 25 in France will be offered free contraception from 2022. It was elaborated that they "would not be charged for medical appointments, tests, or other medical procedures related to birth control" and that this would "cover hormonal contraception, biological tests that go with it, the prescription of contraception and all care related to this contraception".[222]
From August 2022 onwards contraception for women aged between 17 and 25 years will be free in the Republic of Ireland.[223][224]
Public provisioning for contraception
In most parts of the world, the political attitude to contraception determines whether and how much state provisioning of contraceptive care occurs. In the United States, for example, the Republican party and the Democratic party have held opposite positions, contributing to continuous policy shifts over the years.[225][226] In the 2010s, policies, and attitudes to contraceptive care shifted abruptly between Obama's and Trump's administrations.[225] The Trump administration extensively overturned the efforts for contraceptive care, and reduced federal spending, compared to efforts and funding during the Obama administration.[225]
Advocacy
Free the Pill, a collaboration between Advocates for Youth and Ibis Reproductive Health are working to bring birth control over-the-counter, covered by insurance with no age-restriction throughout the United States.[227][228][229]
Approval
On July 13, 2023, the first US daily oral nonprescription over-the-counter birth control pill was approved for manufacturer by the FDA. The pill, Opill is expected to be more effective in preventing unintended pregnancies than condoms are. Opill is expected to be available in 2024 but the price has yet to be set. Perrigo, a pharmaceutical company based in Dublin is the manufacturer.[230]
Research directions
Females
Improvements of existing birth control methods are needed, as around half of those who get pregnant unintentionally are using birth control at the time.[29] A number of alterations of existing contraceptive methods are being studied, including a better female condom, an improved diaphragm, a patch containing only progestin, and a vaginal ring containing long-acting progesterone.[231] This vaginal ring appears to be effective for three or four months and is currently available in some areas of the world.[231] For women who rarely have sex, the taking of the hormonal birth control levonorgestrel around the time of sex looks promising.[232]
A number of methods to perform sterilization via the cervix are being studied. One involves putting quinacrine in the uterus which causes scarring and infertility. While the procedure is inexpensive and does not require surgical skills, there are concerns regarding long-term side effects.[233] Another substance, polidocanol, which functions in the same manner is being looked at.[231] A device called Essure, which expands when placed in the fallopian tubes and blocks them, was approved in the United States in 2002.[233] In 2016, a black boxed warning regarding potentially serious side effects was added,[234][235] and in 2018, the device was discontinued.[236]
Males
Despite high levels of interest in male contraception,[237][238][239] progress been stymied by a lack of industry involvement. Most funding for male contraceptive research is derived from government or philanthropic sources.[240][241][242][243]
A number of novel contraceptive methods based on hormonal and non-hormonal mechanisms of action are in various stages of research and development, up to and including clinical trials,[244][245][246][247][248][249] including gels, pills, injectables, implants, wearables, and oral contraceptives.[250][251][252]
Recent avenues of research include proteins and genes required for male fertility. For instance, the serine/threonine-protein kinase 33 (STK33) is a testis-enriched kinase that is indispensable for male fertility in humans and mice. An inhibitor of this kinase, CDD-2807, has recently been identified and induced reversible male infertility without measurable toxicity in mice.[253] Such an inhibitor would be a potent male contraceptive if it passed safety and efficacy tests.
Animals
Neutering or spaying, which involves removing some of the reproductive organs, is often carried out as a method of birth control in household pets. Many animal shelters require these procedures as part of adoption agreements.[254] In large animals the surgery is known as castration.[255]
Birth control is also being considered as an alternative to hunting as a means of controlling overpopulation in wild animals.[256]Contraceptive vaccines have been found to be effective in a number of different animal populations.[257][258] Kenyan goat herders fix a skirt, called an olor, to male goats to prevent them from impregnating female goats.[259]
^"Definition of Birth control". MedicineNet. Archived from the original on August 6, 2012. Retrieved August 9, 2012.
^ a b c d e f g h iHanson SJ, Burke AE (2010). "Fertility control: contraception, sterilization, and abortion". In Hurt KJ, Guile MW, Bienstock JL, Fox HE, Wallach EE (eds.). The Johns Hopkins manual of gynecology and obstetrics (4th ed.). Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins. pp. 382–395. ISBN 978-1-60547-433-5.
^Oxford English Dictionary. Oxford University Press. 2012.
^World Health Organization (WHO). "Family planning". Health topics. World Health Organization (WHO). Archived from the original on March 18, 2016. Retrieved March 28, 2016.
^Medical eligibility criteria for contraceptive use (Fifth ed.). Geneva, Switzerland: World Health Organization. 2015. ISBN 978-92-4-154915-8. OCLC 932048744.
^Curtis KM, Tepper NK, Jatlaoui TC, Berry-Bibee E, Horton LG, Zapata LB, et al. (July 2016). "U.S. Medical Eligibility Criteria for Contraceptive Use, 2016". MMWR. Recommendations and Reports. 65 (3): 1–103. doi:10.15585/mmwr.rr6503a1. PMID 27467196.
^ a b c d e fWorld Health Organization Department of Reproductive Health and Research (2011). Family planning: A global handbook for providers: Evidence-based guidance developed through worldwide collaboration (PDF) (Rev. and Updated ed.). Geneva: WHO and Center for Communication Programs. ISBN 978-0-9788563-7-3. Archived (PDF) from the original on September 21, 2013.
^Taliaferro LA, Sieving R, Brady SS, Bearinger LH (December 2011). "We have the evidence to enhance adolescent sexual and reproductive health—do we have the will?". Adolescent Medicine. 22 (3): 521–43, xii. PMID 22423463.
^ a bChin HB, Sipe TA, Elder R, Mercer SL, Chattopadhyay SK, Jacob V, et al. (March 2012). "The effectiveness of group-based comprehensive risk-reduction and abstinence education interventions to prevent or reduce the risk of adolescent pregnancy, human immunodeficiency virus, and sexually transmitted infections: two systematic reviews for the Guide to Community Preventive Services". American Journal of Preventive Medicine. 42 (3): 272–94. doi:10.1016/j.amepre.2011.11.006. PMID 22341164.
^ a b c dGizzo S, Fanelli T, Di Gangi S, Saccardi C, Patrelli TS, Zambon A, et al. (October 2012). "Nowadays which emergency contraception? Comparison between past and present: latest news in terms of clinical efficacy, side effects and contraindications". Gynecological Endocrinology. 28 (10): 758–63. doi:10.3109/09513590.2012.662546. PMID 22390259. S2CID 39676240.
^Selected practice recommendations for contraceptive use (2nd ed.). Geneva: World Health Organization. 2004. p. 13. ISBN 978-92-4-156284-3. Archived from the original on September 8, 2017.
^DiCenso A, Guyatt G, Willan A, Griffith L (June 2002). "Interventions to reduce unintended pregnancies among adolescents: systematic review of randomised controlled trials". BMJ. 324 (7351): 1426. doi:10.1136/bmj.324.7351.1426. PMC 115855. PMID 12065267.
^Duffy K, Lynch DA, Santinelli J, Santelli J (December 2008). "Government support for abstinence-only-until-marriage education". Clinical Pharmacology and Therapeutics. 84 (6): 746–8. doi:10.1038/clpt.2008.188. PMID 18923389. S2CID 19499439. Archived from the original on December 11, 2008.
^ a b cBlack AY, Fleming NA, Rome ES (April 2012). "Pregnancy in adolescents". Adolescent Medicine. 23 (1): 123–38, xi. PMID 22764559.
^ a bRowan SP, Someshwar J, Murray P (April 2012). "Contraception for primary care providers". Adolescent Medicine. 23 (1): 95–110, x–xi. PMID 22764557.
^ a b c d eWorld Health Organization Department of Reproductive Health and Research (2011). Family planning: A global handbook for providers: Evidence-based guidance developed through worldwide collaboration (PDF) (Rev. and Updated ed.). Geneva: WHO and Center for Communication Programs. pp. 260–300. ISBN 978-0-9788563-7-3. Archived (PDF) from the original on September 21, 2013.
^Singh S, Darroch JE (June 2012). "Costs and Benefits of Contraceptive Services: Estimates for 2012" (PDF). United Nations Population Fund: 1. Archived (PDF) from the original on August 5, 2012.
^ a bCarr B, Gates MF, Mitchell A, Shah R (July 2012). "Giving women the power to plan their families". Lancet. 380 (9837): 80–82. doi:10.1016/S0140-6736(12)60905-2. PMID 22784540. S2CID 205966410. Archived from the original on May 10, 2013.
^ a b c d e fCleland J, Conde-Agudelo A, Peterson H, Ross J, Tsui A (July 2012). "Contraception and health". Lancet. 380 (9837): 149–156. doi:10.1016/S0140-6736(12)60609-6. PMID 22784533. S2CID 9982712.
^ a bAhmed S, Li Q, Liu L, Tsui AO (July 2012). "Maternal deaths averted by contraceptive use: an analysis of 172 countries". Lancet. 380 (9837): 111–125. doi:10.1016/S0140-6736(12)60478-4. PMID 22784531. S2CID 25724866. Archived from the original on May 10, 2013.
^ a b c dCanning D, Schultz TP (July 2012). "The economic consequences of reproductive health and family planning". Lancet. 380 (9837): 165–171. doi:10.1016/S0140-6736(12)60827-7. PMID 22784535. S2CID 39280999. Archived from the original on June 2, 2013.
^Van Braeckel D, Temmerman M, Roelens K, Degomme O (July 2012). "Slowing population growth for wellbeing and development". Lancet. 380 (9837): 84–85. doi:10.1016/S0140-6736(12)60902-7. PMID 22784542. S2CID 10015998. Archived from the original on May 10, 2013.
^ a b c d e f g h i jTrussell J (May 2011). "Contraceptive failure in the United States". Contraception. 83 (5): 397–404. doi:10.1016/j.contraception.2011.01.021. PMC 3638209. PMID 21477680. Trussell J (2011). "Contraceptive efficacy". In Hatcher RA, Trussell J, Nelson AL, Cates Jr W, Kowal D, Policar MS (eds.). Contraceptive technology (20th revised ed.). New York: Ardent Media. pp. 779–863. ISBN 978-1-59708-004-0. ISSN 0091-9721. OCLC 781956734.
^"U.S. Selected Practice Recommendations for Contraceptive Use, 2013: adapted from the World Health Organization selected practice recommendations for contraceptive use, 2nd edition". MMWR. Recommendations and Reports. 62 (RR-05). Division Of Reproductive Health, National Center for Chronic Disease Prevention Health Promotion, U.S. Centers for Disease Control and Prevention: 1–60. June 2013. PMID 23784109. Archived from the original on July 10, 2013.
^Van der Wijden C, Manion C (October 2015). "Lactational amenorrhoea method for family planning". The Cochrane Database of Systematic Reviews. 2015 (10): CD001329. doi:10.1002/14651858.CD001329.pub2. PMC 6823189. PMID 26457821.
^ a bBlenning CE, Paladine H (December 2005). "An approach to the postpartum office visit". American Family Physician. 72 (12): 2491–2496. PMID 16370405.
^Edlin G, Golanty E, Brown KM (2000). Essentials for health and wellness (2nd ed.). Sudbury, MA: Jones and Bartlett. p. 161. ISBN 978-0-7637-0909-9. Archived from the original on June 10, 2016.
^Edmonds DK, ed. (2012). Dewhurst's textbook of obstetrics & gynaecology (8th ed.). Chichester, West Sussex: Wiley-Blackwell. p. 508. ISBN 978-0-470-65457-6. Archived from the original on May 3, 2016.
^ a b c d e f g h iCunningham FG, Stuart GS (2012). "Contraception and sterilization". In B, Schorge JO, Schaffer JI, Halvorson LM, Bradshaw KD, Cunningham FG (eds.). Williams gynecology (2nd ed.). New York: McGraw-Hill Medical. pp. 132–69. ISBN 978-0-07-171672-7.
^Committee on Adolescence (October 2014). "Contraception for adolescents". Pediatrics. 134 (4): e1244-56. doi:10.1542/peds.2014-2299. PMC 1070796. PMID 25266430.
^Mansour D, Gemzell-Danielsson K, Inki P, Jensen JT (November 2011). "Fertility after discontinuation of contraception: a comprehensive review of the literature". Contraception. 84 (5): 465–77. doi:10.1016/j.contraception.2011.04.002. PMID 22018120.
^ a bMedical eligibility criteria for contraceptive use (PDF) (4th ed.). Geneva: Reproductive Health and Research, World Health Organization. 2009. pp. 1–10. ISBN 978-92-4-156388-8. Archived from the original (PDF) on July 9, 2012.
^Department of Reproductive Health and Research, Family and Community (2004). Selected practice recommendations for contraceptive use (PDF) (2nd ed.). Geneva: World Health Organization. p. Chapter 31. ISBN 978-92-4-156284-3. Archived from the original (PDF) on July 18, 2013.
^Tepper NK, Curtis KM, Steenland MW, Marchbanks PA (May 2013). "Physical examination prior to initiating hormonal contraception: a systematic review". Contraception. 87 (5): 650–4. doi:10.1016/j.contraception.2012.08.010. PMID 23121820.
^ a b c dWorld Health Organization Department of Reproductive Health and Research (2011). Family planning: A global handbook for providers: Evidence-based guidance developed through worldwide collaboration (PDF) (Rev. and Updated ed.). Geneva: WHO and Center for Communication Programs. pp. 1–10. ISBN 978-0-9788563-7-3. Archived (PDF) from the original on September 21, 2013.
^"American Academy of Family Physicians | Choosing Wisely". www.choosingwisely.org. February 24, 2015. Retrieved August 14, 2018.
^Mackenzie J (December 6, 2013). "The male pill? Bring it on". The Guardian. Archived from the original on May 21, 2014. Retrieved May 20, 2014.
^Ammer C (2009). "oral contraceptive". The encyclopedia of women's health (6th ed.). New York: Facts On File. pp. 312–15. ISBN 978-0-8160-7407-5.
^Nelson A, Cwiak C (2011). "Combined oral contraceptives (COCs)". In Hatcher RA, Trussell J, Nelson AL, Cates Jr W, Kowal D, Policar MS (eds.). Contraceptive technology (20th revised ed.). New York: Ardent Media. pp. 249–341 [257–58]. ISBN 978-1-59708-004-0. ISSN 0091-9721. OCLC 781956734.
^ a bHoffman BL (2011). "5 Second-Tier Contraceptive Methods—Very Effective". Williams gynecology (2nd ed.). New York: McGraw-Hill Medical. ISBN 978-0-07-171672-7.
^ a b c dBrito MB, Nobre F, Vieira CS (April 2011). "Hormonal contraception and cardiovascular system". Arquivos Brasileiros de Cardiologia. 96 (4): e81-9. doi:10.1590/S0066-782X2011005000022. PMID 21359483.
^Stegeman BH, de Bastos M, Rosendaal FR, van Hylckama Vlieg A, Helmerhorst FM, Stijnen T, Dekkers OM (September 2013). "Different combined oral contraceptives and the risk of venous thrombosis: systematic review and network meta-analysis". BMJ. 347: f5298. doi:10.1136/bmj.f5298. PMC 3771677. PMID 24030561.
^Kurver MJ, van der Wijden CL, Burgers J (October 4, 2012). "[Summary of the Dutch College of General Practitioners' practice guideline 'Contraception']". Nederlands Tijdschrift voor Geneeskunde (in Dutch). 156 (41): A5083. PMID 23062257.[permanent dead link]
^Tosetto A, Iorio A, Marcucci M, Baglin T, Cushman M, Eichinger S, et al. (June 2012). "Predicting disease recurrence in patients with previous unprovoked venous thromboembolism: a proposed prediction score (DASH)". Journal of Thrombosis and Haemostasis. 10 (6): 1019–25. doi:10.1111/j.1538-7836.2012.04735.x. PMID 22489957. S2CID 27149654.
^Burrows LJ, Basha M, Goldstein AT (September 2012). "The effects of hormonal contraceptives on female sexuality: a review". The Journal of Sexual Medicine. 9 (9): 2213–23. doi:10.1111/j.1743-6109.2012.02848.x. PMID 22788250.
^ a bShulman LP (October 2011). "The state of hormonal contraception today: benefits and risks of hormonal contraceptives: combined estrogen and progestin contraceptives". American Journal of Obstetrics and Gynecology. 205 (4 Suppl): S9-13. doi:10.1016/j.ajog.2011.06.057. PMID 21961825.
^Havrilesky LJ, Moorman PG, Lowery WJ, Gierisch JM, Coeytaux RR, Urrutia RP, et al. (July 2013). "Oral contraceptive pills as primary prevention for ovarian cancer: a systematic review and meta-analysis". Obstetrics and Gynecology. 122 (1): 139–47. doi:10.1097/AOG.0b013e318291c235. PMID 23743450. S2CID 31552437.
^Mantha S, Karp R, Raghavan V, Terrin N, Bauer KA, Zwicker JI (August 2012). "Assessing the risk of venous thromboembolic events in women taking progestin-only contraception: a meta-analysis". BMJ. 345 (aug07 2): e4944. doi:10.1136/bmj.e4944. PMC 3413580. PMID 22872710.
^Burke AE (October 2011). "The state of hormonal contraception today: benefits and risks of hormonal contraceptives: progestin-only contraceptives". American Journal of Obstetrics and Gynecology. 205 (4 Suppl): S14-7. doi:10.1016/j.ajog.2011.04.033. PMID 21961819.
^Rott H (August 2012). "Thrombotic risks of oral contraceptives". Current Opinion in Obstetrics & Gynecology. 24 (4): 235–40. doi:10.1097/GCO.0b013e328355871d. PMID 22729096. S2CID 23938634.
^ a bNeinstein L (2008). Adolescent health care : a practical guide (5th ed.). Philadelphia: Lippincott Williams & Wilkins. p. 624. ISBN 978-0-7817-9256-1. Archived from the original on June 17, 2016.
^Chaudhuri SK (2007). "Barrier Contraceptives". Practice Of Fertility Control: A Comprehensive Manual (7th ed.). Elsevier India. p. 88. ISBN 978-81-312-1150-2. Archived from the original on April 30, 2016.
^ a bHamilton R (2012). Pharmacology for nursing care (8th ed.). St. Louis, MO: Elsevier/Saunders. p. 799. ISBN 978-1-4377-3582-6. Archived from the original on June 3, 2016.
^Facts for life (4th ed.). New York: United Nations Children's Fund. 2010. p. 141. ISBN 978-92-806-4466-1. Archived from the original on May 13, 2016.
^Pray WS (2005). Nonprescription product therapeutics (2nd ed.). Philadelphia: Lippincott Williams & Wilkins. p. 414. ISBN 978-0-7817-3498-1. Archived from the original on April 30, 2016.
^Committee on Adolescence (November 2013). "Condom Use by Adolescents". Pediatrics. 132 (5): 973–981. doi:10.1542/peds.2013-2821. PMID 28448257.
^Eberhard N (2010). Andrology Male Reproductive Health and Dysfunction (3rd ed.). [S.l.]: Springer-Verlag Berlin Heidelberg. p. 563. ISBN 978-3-540-78355-8. Archived from the original on May 10, 2016.
^Barbieri JF (2009). Yen and Jaffe's reproductive endocrinology : physiology, pathophysiology, and clinical management (6th ed.). Philadelphia: Saunders/Elsevier. p. 873. ISBN 978-1-4160-4907-4. Archived from the original on May 18, 2016.
^"Preventing Sexually Transmitted Infections (STIs)". British Columbia Health Link. February 2017. Archived from the original on July 27, 2020. Retrieved March 31, 2018.
^Kuyoh MA, Toroitich-Ruto C, Grimes DA, Schulz KF, Gallo MF (January 2003). "Sponge versus diaphragm for contraception: a Cochrane review". Contraception. 67 (1): 15–8. doi:10.1016/s0010-7824(02)00434-1. PMID 12521652.
^Medical eligibility criteria for contraceptive use (4th ed.). Geneva: Reproductive Health and Research, World Health Organization. 2009. p. 88. ISBN 978-92-4-156388-8. Archived from the original on May 15, 2016.
^Winner B, Peipert JF, Zhao Q, Buckel C, Madden T, Allsworth JE, Secura GM (May 2012). "Effectiveness of long-acting reversible contraception". The New England Journal of Medicine. 366 (21): 1998–2007. doi:10.1056/NEJMoa1110855. PMID 22621627. S2CID 16812353.
^Hanson SJ, Burke AE (March 28, 2012). "Fertility Control: Contraception, Sterilization, and Abortion". In Hurt KJ, Guile MW, Bienstock JL, Fox HE, Wallach EE (eds.). The Johns Hopkins manual of gynecology and obstetrics (4th ed.). Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins. p. 232. ISBN 978-1-60547-433-5. Archived from the original on May 12, 2016.
^ a bCommittee on Adolescent Health Care Long-Acting Reversible Contraception Working Group, The American College of Obstetricians and Gynecologists (October 2012). "Committee opinion no. 539: adolescents and long-acting reversible contraception: implants and intrauterine devices". Obstetrics and Gynecology. 120 (4): 983–8. doi:10.1097/AOG.0b013e3182723b7d. PMID 22996129. S2CID 35516759.
^ a bSperoff L, Darney PD (2010). A clinical guide for contraception (5th ed.). Philadelphia: Lippincott Williams & Wilkins. pp. 242–43. ISBN 978-1-60831-610-6. Archived from the original on May 6, 2016.
^Black K, Lotke P, Buhling KJ, Zite NB (October 2012). "A review of barriers and myths preventing the more widespread use of intrauterine contraception in nulliparous women". The European Journal of Contraception & Reproductive Health Care. 17 (5): 340–50. doi:10.3109/13625187.2012.700744. PMC 4950459. PMID 22834648.
^ a b cGabbe S (2012). Obstetrics: Normal and Problem Pregnancies. Elsevier Health Sciences. p. 527. ISBN 978-1-4557-3395-8. Archived from the original on May 15, 2016.
^Steenland MW, Tepper NK, Curtis KM, Kapp N (November 2011). "Intrauterine contraceptive insertion postabortion: a systematic review". Contraception. 84 (5): 447–64. doi:10.1016/j.contraception.2011.03.007. PMID 22018119.
^Roe AH, Bartz D (January 2019). "Society of Family Planning clinical recommendations: contraception after surgical abortion". Contraception. 99 (1): 2–9. doi:10.1016/j.contraception.2018.08.016. PMID 30195718.
^Falcone T, Hurd WW, eds. (2007). Clinical reproductive medicine and surgery. Philadelphia: Mosby. p. 409. ISBN 978-0-323-03309-1. Archived from the original on June 17, 2016.
^Grimes DA (2007). "Intrauterine Devices (IUDs)". In Hatcher RA, Nelson TJ, Guest F, Kowal D (eds.). Contraceptive Technology (19th ed.).
^ a b cMarnach ML, Long ME, Casey PM (March 2013). "Current issues in contraception". Mayo Clinic Proceedings. 88 (3): 295–9. doi:10.1016/j.mayocp.2013.01.007. PMID 23489454.
^"Popularity Disparity: Attitudes About the IUD in Europe and the United States". Guttmacher Policy Review. 2007. Archived from the original on March 7, 2010. Retrieved April 27, 2010.
^Cramer DW (February 2012). "The epidemiology of endometrial and ovarian cancer". Hematology/Oncology Clinics of North America. 26 (1): 1–12. doi:10.1016/j.hoc.2011.10.009. PMC 3259524. PMID 22244658.
^Adams CE, Wald M (August 2009). "Risks and complications of vasectomy". The Urologic Clinics of North America. 36 (3): 331–6. doi:10.1016/j.ucl.2009.05.009. PMID 19643235.
^Hillard PA (2008). The 5-minute obstetrics and gynecology consult. Hagerstwon, MD: Lippincott Williams & Wilkins. p. 265. ISBN 978-0-7817-6942-6. Archived from the original on June 11, 2016.
^"Vasectomy Guideline – American Urological Association". www.auanet.org. Retrieved October 26, 2021.
^Hillard PA (2008). The 5-minute obstetrics and gynecology consult. Hagerstwon, MD: Lippincott Williams & Wilkins. p. 549. ISBN 978-0-7817-6942-6. Archived from the original on May 5, 2016.
^Lee Goldman, Andrew I. Schafer, eds. (2020). "Contraception". Goldman-Cecil medicine (26th ed.). Philadelphia, PA: Elsevier. pp. 1568–1575. ISBN 978-0-323-53266-2. OCLC 1118693594.
^Fahim, M. S., et al. "Heat in male contraception (hot water 60°C, infrared, microwave, and ultrasound)." Contraception 11.5 (1975): 549–562.
^Fahim, M. S., et al. "Ultrasound as a new method of male contraception." Fertility and sterility 28.8 (1977): 823–831.
^Fahim, M. S., Z. Fahim, and F. Azzazi. "Effect of ultrasound on testicular electrolytes (sodium and potassium)." Archives of andrology 1.2 (1978): 179–184.
^Lonidamine analogues for fertility management, WO2011005759A3
WIPO (PCT), Ingrid Gunda GeorgeJoseph S. TashRamappa ChakrsaliSudhakar R. JakkarajJames P. Calvet
^United States Patent US3934015A, Oral male antifertility method and compositions
^Hillis SD, Marchbanks PA, Tylor LR, Peterson HB (June 1999). "Poststerilization regret: findings from the United States Collaborative Review of Sterilization". Obstetrics and Gynecology. 93 (6): 889–895. doi:10.1016/s0029-7844(98)00539-0. PMID 10362150. S2CID 38389864.
^Hatcher R (2008). Contraceptive technology (19th ed.). New York: Ardent Media. p. 390. ISBN 978-1-59708-001-9. Archived from the original on May 6, 2016.
^Moore DS (2010). The basic practice of statistics (5th ed.). New York: Freeman. p. 25. ISBN 978-1-4292-2426-0. Archived from the original on April 27, 2016.
^ a b cDeffieux X, Morin Surroca M, Faivre E, Pages F, Fernandez H, Gervaise A (May 2011). "Tubal anastomosis after tubal sterilization: a review". Archives of Gynecology and Obstetrics. 283 (5): 1149–58. doi:10.1007/s00404-011-1858-1. PMID 21331539. S2CID 28359350.
^ a bShridharani A, Sandlow JI (November 2010). "Vasectomy reversal versus IVF with sperm retrieval: which is better?". Current Opinion in Urology. 20 (6): 503–9. doi:10.1097/MOU.0b013e32833f1b35. PMID 20852426. S2CID 42105503.
^Nagler HM, Jung H (August 2009). "Factors predicting successful microsurgical vasectomy reversal". The Urologic Clinics of North America. 36 (3): 383–90. doi:10.1016/j.ucl.2009.05.010. PMID 19643240.
^ a b c dGrimes DA, Gallo MF, Grigorieva V, Nanda K, Schulz KF (October 2004). "Fertility awareness-based methods for contraception". The Cochrane Database of Systematic Reviews. 2012 (4): CD004860. doi:10.1002/14651858.CD004860.pub2. PMC 8855505. PMID 15495128.
^Lawrence R (2010). Breastfeeding : a guide for the medical professional (7th ed.). Philadelphia: Saunders. p. 673. ISBN 978-1-4377-0788-5.
^ a bFreundl G, Sivin I, Batár I (April 2010). "State-of-the-art of non-hormonal methods of contraception: IV. Natural family planning". The European Journal of Contraception & Reproductive Health Care. 15 (2): 113–23. doi:10.3109/13625180903545302. PMID 20141492. S2CID 207523506.
^Jennings VH, Burke AE (November 1, 2011). "Fertility awareness-based methods". In Hatcher RA, Trussell J, Nelson AL, Cates Jr W, Kowal D, Policar MS (eds.). Contraceptive technology (20th revised ed.). New York: Ardent Media. pp. 417–34. ISBN 978-1-59708-004-0. ISSN 0091-9721. OCLC 781956734.
^Mangone ER, Lebrun V, Muessig KE (January 2016). "Mobile Phone Apps for the Prevention of Unintended Pregnancy: A Systematic Review and Content Analysis". JMIR mHealth and uHealth. 4 (1): e6. doi:10.2196/mhealth.4846. PMC 4738182. PMID 26787311.
^ a bMedical eligibility criteria for contraceptive use (PDF) (4th ed.). Geneva: Reproductive Health and Research, World Health Organization. 2009. pp. 91–100. ISBN 978-92-4-156388-8. Archived from the original (PDF) on July 9, 2012.
^ a bJones RK, Fennell J, Higgins JA, Blanchard K (June 2009). "Better than nothing or savvy risk-reduction practice? The importance of withdrawal". Contraception. 79 (6): 407–10. doi:10.1016/j.contraception.2008.12.008. PMID 19442773.
^Killick SR, Leary C, Trussell J, Guthrie KA (March 2011). "Sperm content of pre-ejaculatory fluid". Human Fertility. 14 (1): 48–52. doi:10.3109/14647273.2010.520798. PMC 3564677. PMID 21155689.
^ a b"Abstinence". Planned Parenthood. 2009. Archived from the original on September 10, 2009. Retrieved September 9, 2009.
^Murthy AS, Harwood B (2007). "Contraception Update". Primary Care in Obstetrics and Gynecology (2nd ed.). New York: Springer. pp. 241–264. doi:10.1007/978-0-387-32328-2_12. ISBN 978-0-387-32327-5.
^Alters S, Schiff W (October 5, 2009). Essential Concepts for Healthy Living. Jones & Bartlett Publishers. p. 116. ISBN 978-0-7637-5641-3. Retrieved December 30, 2017.
^Greenberg JS, Bruess CE, Oswalt SB (2016). Exploring the Dimensions of Human Sexuality. Jones & Bartlett Publishers. p. 191. ISBN 978-1-4496-9801-0. Retrieved December 30, 2017.
^Fortenberry JD (April 2005). "The limits of abstinence-only in preventing sexually transmitted infections". The Journal of Adolescent Health. 36 (4): 269–70. doi:10.1016/j.jadohealth.2005.02.001. PMID 15780781.
^Best K (2005). "Nonconsensual Sex Undermines Sexual Health". Network. 23 (4). Archived from the original on February 18, 2009.
^Thomas RM (2009). Sex and the American teenager seeing through the myths and confronting the issues. Lanham, MD: Rowman & Littlefield Education. p. 81. ISBN 978-1-60709-018-2.
^Edlin G (2012). Health & Wellness. Jones & Bartlett Learning. p. 213. ISBN 978-1-4496-3647-0.
^ a bSantelli JS, Kantor LM, Grilo SA, Speizer IS, Lindberg LD, Heitel J, et al. (September 2017). "Abstinence-Only-Until-Marriage: An Updated Review of U.S. Policies and Programs and Their Impact". The Journal of Adolescent Health. 61 (3): 273–280. doi:10.1016/j.jadohealth.2017.05.031. hdl:1805/15683. PMID 28842065.
^Kowal D (2007). "Abstinence and the Range of Sexual Expression". In Hatcher RA, et al. (eds.). Contraceptive Technology (19th rev. ed.). New York: Ardent Media. pp. 81–86. ISBN 978-0-9664902-0-6.
^Blackburn ST (2007). Maternal, fetal, & neonatal physiology : a clinical perspective (3rd ed.). St. Louis, MO: Saunders Elsevier. p. 157. ISBN 978-1-4160-2944-1. Archived from the original on May 12, 2016.
^"WHO 10 facts on breastfeeding". World Health Organization. April 2005. Archived from the original on June 23, 2013.
^Van der Wijden C, Manion C (October 2015). "Lactational amenorrhoea method for family planning". The Cochrane Database of Systematic Reviews. 2015 (10): CD001329. doi:10.1002/14651858.CD001329.pub2. PMC 6823189. PMID 26457821.
^ a b cFritz M (2012). Clinical Gynecologic Endocrinology and Infertility. Lippincott Williams & Wilkins. pp. 1007–08. ISBN 978-1-4511-4847-3. Archived from the original on June 3, 2016.
^Swisher J, Lauwers A (October 25, 2010). Counseling the nursing mother a lactation consultant's guide (5th ed.). Sudbury, MA: Jones & Bartlett Learning. pp. 465–66. ISBN 978-1-4496-1948-0. Archived from the original on June 16, 2016.
^Office of Population Research, Association of Reproductive Health Professionals (July 31, 2013). "What is the difference between emergency contraception, the 'morning after pill', and the 'day after pill'?". Princeton: Princeton University. Archived from the original on September 23, 2013. Retrieved September 7, 2013.
^ a bLeung VW, Levine M, Soon JA (February 2010). "Mechanisms of action of hormonal emergency contraceptives". Pharmacotherapy. 30 (2): 158–68. doi:10.1592/phco.30.2.158. PMID 20099990. S2CID 41337748. The evidence strongly supports disruption of ovulation as a mechanism of action. The data suggest that emergency contraceptives are unlikely to act by interfering with implantation
^ a b c dShen J, Che Y, Showell E, Chen K, Cheng L, et al. (Cochrane Fertility Regulation Group) (January 2019). "Interventions for emergency contraception". The Cochrane Database of Systematic Reviews. 1 (1): CD001324. doi:10.1002/14651858.CD001324.pub6. PMC 7055045. PMID 30661244.
^Kripke C (September 2007). "Advance provision for emergency oral contraception". American Family Physician. 76 (5): 654. PMID 17894132.
^Shrader SP, Hall LN, Ragucci KR, Rafie S (September 2011). "Updates in hormonal emergency contraception". Pharmacotherapy. 31 (9): 887–95. doi:10.1592/phco.31.9.887. PMID 21923590. S2CID 33900390.
^Beeston A (January 27, 2022). "Pharmacists gave the POP with emergency contraception". NIHR Evidence. doi:10.3310/alert_48882. Retrieved May 31, 2024.
^Cameron ST, Glasier A, McDaid L, Radley A, Patterson S, Baraitser P, Stephenson J, Gilson R, Battison C, Cowle K, Vadiveloo T, Johnstone A, Morelli A, Goulao B, Forrest M (May 5, 2021). "Provision of the progestogen-only pill by community pharmacies as bridging contraception for women receiving emergency contraception: the Bridge-it RCT". Health Technology Assessment. 25 (27): 1–92. doi:10.3310/hta25270. hdl:2164/16696. ISSN 2046-4924.
^Richardson AR, Maltz FN (January 2012). "Ulipristal acetate: review of the efficacy and safety of a newly approved agent for emergency contraception". Clinical Therapeutics. 34 (1): 24–36. doi:10.1016/j.clinthera.2011.11.012. PMID 22154199.
^"Update on Emergency Contraception". Association of Reproductive Health Professionals. March 2011. Archived from the original on May 11, 2013. Retrieved May 20, 2013.
^Cleland K, Zhu H, Goldstuck N, Cheng L, Trussell J (July 2012). "The efficacy of intrauterine devices for emergency contraception: a systematic review of 35 years of experience". Human Reproduction. 27 (7): 1994–2000. doi:10.1093/humrep/des140. PMC 3619968. PMID 22570193.
^Glasier A, Cameron ST, Blithe D, Scherrer B, Mathe H, Levy D, et al. (October 2011). "Can we identify women at risk of pregnancy despite using emergency contraception? Data from randomized trials of ulipristal acetate and levonorgestrel". Contraception. 84 (4): 363–7. doi:10.1016/j.contraception.2011.02.009. PMID 21920190.
^"Dual protection against unwanted pregnancy and HIV / STDs". Sexual Health Exchange (3): 8. 1998. PMID 12294688.
^ a bCates W, Steiner MJ (March 2002). "Dual protection against unintended pregnancy and sexually transmitted infections: what is the best contraceptive approach?". Sexually Transmitted Diseases. 29 (3): 168–74. doi:10.1097/00007435-200203000-00007. PMID 11875378. S2CID 42792667.
^Farber NA, Farber NA (May 2000). "Statement on Dual Protection against Unwanted Pregnancy and Sexually Transmitted Infections, including HIV". Terapevticheskii Arkhiv. 53 (10). International Planned Parenthood Federation: 135–140. Archived from the original on April 10, 2016.
^Gupta RC (2011). Reproductive and Developmental Toxicology. Academic Press. p. 105. ISBN 978-0-12-382032-7. Archived from the original on May 16, 2016.
^Bhakta J, Bainbridge J, Borgelt L (November 2015). "Teratogenic medications and concurrent contraceptive use in women of childbearing ability with epilepsy". Epilepsy & Behavior. 52 (Pt A): 212–7. doi:10.1016/j.yebeh.2015.08.004. PMID 26460786. S2CID 6504198.
^ a bSholapurkar SL (February 2010). "Is there an ideal interpregnancy interval after a live birth, miscarriage or other adverse pregnancy outcomes?". Journal of Obstetrics and Gynaecology. 30 (2): 107–10. doi:10.3109/01443610903470288. PMID 20143964. S2CID 6346721.
^Lavin C, Cox JE (August 2012). "Teen pregnancy prevention: current perspectives". Current Opinion in Pediatrics. 24 (4): 462–9. doi:10.1097/MOP.0b013e3283555bee. PMID 22790099. S2CID 12022584.
^ a b cRobbins CL, Ott MA (October 2017). "Contraception options and provision to adolescents". Minerva Pediatrica. 69 (5): 403–414. doi:10.23736/s0026-4946.17.05026-5. hdl:1805/14082. PMID 28643995.
^ a bBritton LE, Alspaugh A, Greene MZ, McLemore MR (February 2020). "CE: An Evidence-Based Update on Contraception". The American Journal of Nursing. 120 (2): 22–33. doi:10.1097/01.NAJ.0000654304.29632.a7. PMC 7533104. PMID 31977414.
^ a b cTsui AO, McDonald-Mosley R, Burke AE (April 2010). "Family planning and the burden of unintended pregnancies". Epidemiologic Reviews. 32 (1): 152–74. doi:10.1093/epirev/mxq012. PMC 3115338. PMID 20570955.
^ a bRosenthal E (June 30, 2013). "American Way of Birth, Costliest in the World". New York Times. Archived from the original on March 14, 2017.
^"Expenditures on Children by Families, 2011". United States Department of Agriculture, Center for Nutrition Policy and Promotion. Archived from the original on March 8, 2008. Retrieved August 29, 2012.
^"Demand for family planning satisfied by modern methods". Our World in Data. Retrieved March 5, 2020.
^ a b c d e fDarroch JE (March 2013). "Trends in contraceptive use". Contraception. 87 (3): 259–63. doi:10.1016/j.contraception.2012.08.029. PMID 23040137.
^Darney L, Speroff PD (2010). A clinical guide for contraception (5th ed.). Philadelphia: Lippincott Williams & Wilkins. p. 315. ISBN 978-1-60831-610-6.
^Naz RK, Rowan S (June 2009). "Update on male contraception". Current Opinion in Obstetrics & Gynecology. 21 (3): 265–9. doi:10.1097/gco.0b013e328329247d. PMID 19469045. S2CID 40507937.
^Cleland JG, Ndugwa RP, Zulu EM (February 2011). "Family planning in sub-Saharan Africa: progress or stagnation?". Bulletin of the World Health Organization. 89 (2): 137–43. doi:10.2471/BLT.10.077925. PMC 3040375. PMID 21346925.
^ a bDarroch JE, Singh S (May 2013). "Trends in contraceptive need and use in developing countries in 2003, 2008, and 2012: an analysis of national surveys". Lancet. 381 (9879): 1756–62. doi:10.1016/S0140-6736(13)60597-8. PMID 23683642. S2CID 8257042.
^ a bRasch V (July 2011). "Unsafe abortion and postabortion care – an overview". Acta Obstetricia et Gynecologica Scandinavica. 90 (7): 692–700. doi:10.1111/j.1600-0412.2011.01165.x. PMID 21542813. S2CID 27737728.
^ a b cCuomo A (2010). "Birth control". In O'Reilly A (ed.). Encyclopedia of motherhood. Thousand Oaks, CA: Sage Publications. pp. 121–26. ISBN 978-1-4129-6846-1.
^Lipsey RG, Carlaw K, Bekar C (2005). "Historical Record on the Control of Family Size". Economic Transformations: General Purpose Technologies and Long-Term Economic Growth. Oxford University Press. pp. 335–40. ISBN 978-0-19-928564-8.
^ a bunspecified (2001). "Herbal contraceptives and abortifacients". In Bullough VL (ed.). Encyclopedia of birth control. Santa Barbara, CA: ABC-CLIO. pp. 125–28. ISBN 978-1-57607-181-6.
^Totelin LM (2009). Hippocratic Recipes: Oral and Written Transmission of Pharmacological Knowledge in Fifth- and Fourth-Century Greece. Leiden, Netherlands; Boston: Brill. pp. 158–61. ISBN 978-90-04-17154-1.
^ a b c d e f gCarrick PJ (2001). Medical Ethics in Ancient World. Washington, DC: Georgetown University Press. pp. 119–22. ISBN 978-1-58901-861-7.
^McTavish L (2007). "Contraception and birth control". In Robin D (ed.). Encyclopedia of women in the Renaissance : Italy, France, and England. Santa Barbara, CA: ABC-CLIO. pp. 91–92. ISBN 978-1-85109-772-2.
^ a b c"A History of Birth Control Methods" (PDF). Planned Parenthood Report. January 2012. Archived (PDF) from the original on November 6, 2015.
^Hartmann B (1997). "Population control I: Birth of an ideology". International Journal of Health Services. 27 (3): 523–40. doi:10.2190/bl3n-xajx-0yqb-vqbx. PMID 9285280. S2CID 39035850.
^Simms M (January 27, 1977). "Review: A History of the Malthusian League 1877–1927". New Scientist. Archived from the original on May 5, 2016.
^d'Arcy F (November 1977). "The Malthusian League and the resistance to birth control propaganda in late Victorian Britain". Population Studies. 31 (3): 429–48. doi:10.2307/2173367. JSTOR 2173367. PMID 11630505.
^Meyer JE (2004). Any friend of the movement: networking for birth control, 1920–1940. Ohio State University Press. p. 184. ISBN 978-0-8142-0954-7. Archived from the original on January 3, 2014.
^Galvin R (1998). "Margaret Sanger's "Deeds of Terrible Virtue"". National Endowment for the Humanities. Archived from the original on October 1, 2013. Retrieved January 27, 2014.
^Rossi A (1988). The Feminist Papers. Boston: Northeastern University Press. p. 523. ISBN 978-1-55553-028-0.
^ a b c"Biographical Sketch". About Sanger. New York University. Archived from the original on June 28, 2017. Retrieved February 24, 2017.
^Pastorello K (2013). The Progressives: Activism and Reform in American Society, 1893–1917. John Wiley & Sons. p. 65. ISBN 978-1-118-65112-4. Archived from the original on June 4, 2016.
^Zorea A (2012). Birth Control. Santa Barbara, CA: Greenwood. p. 43. ISBN 978-0-313-36254-5.
^Baker JH (2012). Margaret Sanger : a life of passion (First pbk. ed.). Farrar, Straus and Giroux. pp. 115–17. ISBN 978-1-4299-6897-3. Archived from the original on May 4, 2016.
^McCann CR (2010). "Women as Leaders in the Contraceptive Movement". In O'Connor K (ed.). Gender and Women's Leadership: A Reference Handbook. Sage. p. 751. ISBN 978-1-84885-583-0. OCLC 568741234. Archived from the original on June 10, 2016.
^Küenzl J, Schwabenland C, Elmaco J, Hale S, Levi E, Chen M, et al. (2010), "International Planned Parenthood Federation", International Encyclopedia of Civil Society, pp. 891–892, doi:10.1007/978-0-387-93996-4_403, ISBN 978-0-387-93994-0
^ a b"The Bitter Pill: Harvard and the Dark History of Birth Control | Magazine | The Harvard Crimson". www.thecrimson.com. Retrieved December 14, 2021.
^Seaman B (2003). The greatest experiment ever performed on women : exploding the estrogen myth. New York: Hyperion. ISBN 978-0-7868-6853-7. OCLC 52515011.
^"Puerto Ricans recall being guinea pigs for 'magic pill'". Chicago Tribune. April 11, 2004. Retrieved December 14, 2021.
^ a b cBuenker JD, Kantowicz ER, eds. (1988). Historical dictionary of the Progressive Era, 1890–1920. New York: Greenwood Press. ISBN 978-0313243097. OCLC 17807492.
^McGerr M (2014). A fierce discontent : the rise and fall of the progressive movement in a. Free Press. ISBN 9781439136034. OCLC 893124592.
^Hall R (1977). Passionate Crusader. Harcourt, Brace, Jovanovich. p. 186. ISBN 9780151712885.
^Stopes MC (1925). The First Five Thousand. London: John Bale, Sons & Danielsson. p. 9. OCLC 12690936.
^ a b"Family Planning Timeline". Congressional Digest. 2015.
^Herbert M (September 5, 2012). "Salford's birth control pioneers". The Guardian. Archived from the original on May 28, 2015. Retrieved May 28, 2015.
^Hall L (2011). The life and times of Stella Browne : feminist and free spirit. London: I.B. Tauris. p. 173. ISBN 978-1-84885-583-0.
^BCIC Memorandum on Proposed Re-organisation [c. 1931]. Wellcome Library, Archives of the Eugenics Society (WL/SA/EUG/D/12/12.)
^Wright H (1935). Birth Control: Advice on Family Spacing and Healthy Sex Life. London: Cassell's Health Handbooks.
^Szuhan N (September 2018). "Sex in the laboratory: the Family Planning Association and contraceptive science in Britain, 1929–1959". British Journal for the History of Science. 51 (3): 487–510. doi:10.1017/S0007087418000481. PMID 29952279. S2CID 49474491.
^Birth Control Investigation Committee Statement of Intent [c.1927], Wellcome Library, Archives of the Family Planning Association (WL/SA/FPA), WL/SA/FPA/A13/5.
^Bailey MJ (2013). "Fifty Years of Family Planning: New Evidence on the Long-Run Effects of Increasing Access to Contraception". Brookings Papers on Economic Activity. 2013: 341–409. doi:10.1353/eca.2013.0001. ISSN 0007-2303. PMC 4203450. PMID 25339778.
^"Public Attitudes about Birth Control | Roper Center for Public Opinion Research". ropercenter.cornell.edu. Retrieved December 19, 2023.
^"BIRTH CONTROL AID AT PEAK IN NATION; 374 Clinics Now Operating, an Increase of 87 in a Year, League Reports". The New York Times. January 27, 1938. ISSN 0362-4331. Retrieved June 21, 2022.
^Doan A (2007). Opposition and Intimidation: The Abortion Wars and Strategies of Political Harassment. University of Michigan Press. pp. 53–54. ISBN 978-0-472-06975-0.
^"Griswold v. Connecticut: Landmark Case Remembered", by Andi Reardon. NY Times, May 28, 1989
^"Catherine Roraback, 87, Influential Lawyer, Dies" by Dennis Hevesi Oct. 20, 2007.
^"History of Birth Control in the United States". Congressional Digest. 2012.
^"Birth control benefits and reproductive health care options in the Health Insurance Marketplace". HealthCare.gov. Archived from the original on February 12, 2016. Retrieved February 17, 2016.
^Fritz MA, Speroff L (2011). "Intrauterine contraception". Clinical gynecologic endocrinology and infertility (8th ed.). Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins. pp. 1095–98. ISBN 978-0-7817-7968-5. Archived from the original on November 16, 2016.
^"American Experience | The Pill | Timeline". www.pbs.org. Archived from the original on October 1, 2016. Retrieved October 20, 2016.
^Poston D (2010). Population and Society: An Introduction to Demography. Cambridge University Press. p. 98. ISBN 978-1-139-48938-6. Archived from the original on November 16, 2016.
^Zhang J, Zhou K, Shan D, Luo X (May 2022). "Medical methods for first trimester abortion". The Cochrane Database of Systematic Reviews. 2022 (5): CD002855. doi:10.1002/14651858.CD002855.pub5. PMC 9128719. PMID 35608608.
^Cottingham J, Germain A, Hunt P (July 2012). "Use of human rights to meet the unmet need for family planning". Lancet. 380 (9837): 172–80. doi:10.1016/S0140-6736(12)60732-6. PMID 22784536. S2CID 41854959.
^Doan A (2007). Opposition and Intimidation: The Abortion Wars and Strategies of Political Harassment. University of Michigan Press. pp. 62–63. ISBN 978-0-472-06975-0.
^Singh S, Darroch JE (June 2012). "Adding It Up: Costs and Benefits of Contraceptive Services Estimates for 2012" (PDF). Guttmacher Institute and United Nations Population Fund (UNFPA), 201. Archived (PDF) from the original on August 5, 2012.
^ACOG (September 9, 2014). "ACOG Statement on OTC Access to Contraception". Archived from the original on September 10, 2014. Retrieved September 11, 2014.
^Garner AC, Michel AR (November 4, 2016). ""The Birth Control Divide": U.S. Press Coverage of Contraception, 1873–2013". Journalism & Communication Monographs. 18 (4): 180–234. doi:10.1177/1522637916672457. S2CID 151781215.
^Srikanthan A, Reid RL (February 2008). "Religious and cultural influences on contraception". Journal of Obstetrics and Gynaecology Canada. 30 (2): 129–137. doi:10.1016/s1701-2163(16)32736-0. PMID 18254994.
^Pope Paul VI (July 25, 1968). "Humanae Vitae: Encyclical of Pope Paul VI on the Regulation of Birth". Vatican. Archived from the original on August 24, 2000. Retrieved October 1, 2006.
^Ruether RR (2006). "Women in North American Catholicism". In Keller RS (ed.). Encyclopedia of women and religion in North America. Bloomington, IN [u.a.]: Indiana Univ. Press. p. 132. ISBN 978-0-253-34686-5. Archived from the original on May 29, 2016.
^Digby B, Ferretti J, Flintoff I, Owen A, Ryan C (2001). Digby B (ed.). Heinemann 16–19 Geography: Global Challenges Student Book (2nd ed.). Heinemann. p. 158. ISBN 978-0-435-35249-3. Archived from the original on May 12, 2016.
^Rengel M (2000). Encyclopedia of birth control. Phoenix, AZ: Oryx Press. p. 202. ISBN 978-1-57356-255-3. Archived from the original on June 3, 2016.
^Harakas SS (August 12, 1985). "The Stand of the Orthodox Church on Controversial Issues – Society Articles – Greek Orthodox Archdiocese of America". Greek Orthodox Archdiocese of America. Retrieved September 5, 2019.
^Bennett JA (2008). Water is thicker than blood : an Augustinian theology of marriage and singleness. Oxford: Oxford University Press. p. 178. ISBN 978-0-19-531543-1. Archived from the original on May 28, 2016.
^Feldman DM (1998). Birth Control in Jewish Law. Lanham, MD: Jason Aronson. ISBN 978-0-7657-6058-6.
^"Hindu Beliefs and Practices Affecting Health Care". University of Virginia Health System. Archived from the original on March 23, 2004. Retrieved October 6, 2006.
^"More Questions & Answers on Buddhism: Birth Control and Abortion". Alan Khoo. Archived from the original on June 29, 2008. Retrieved June 14, 2008.
^Akbar KF. "Family Planning and Islam: A Review". Hamdard Islamicus. XVII (3). Archived from the original on September 26, 2006.
^ a b"World Contraception Day". Archived from the original on August 18, 2014.
^Hutcherson H (2002). What your mother never told you about s.e.x (1st Perigee ed.). New York: Perigee Book. p. 201. ISBN 978-0-399-52853-8. Archived from the original on June 29, 2016.
^Rengel M (2000). Encyclopedia of birth control. Phoenix, AZ: Oryx Press. p. 65. ISBN 978-1-57356-255-3. Archived from the original on May 6, 2016.
^Cottrell BH (March–April 2010). "An updated review of evidence to discourage douching". MCN: The American Journal of Maternal/Child Nursing. 35 (2): 102–7, quiz 108–9. doi:10.1097/NMC.0b013e3181cae9da. PMID 20215951. S2CID 46715131.
^Alexander W (2013). New Dimensions In Women's Health – Book Alone (6th ed.). Jones & Bartlett Publishers. p. 105. ISBN 978-1-4496-8375-7. Archived from the original on May 6, 2016.
^Sharkey H (2013). Need to Know Fertility and Conception and Pregnancy. HarperCollins. p. 17. ISBN 978-0-00-751686-5. Archived from the original on June 3, 2016.
^Strange M (2011). Encyclopedia of women in today's world. Thousand Oaks, CA: Sage Reference. p. 928. ISBN 978-1-4129-7685-5. Archived from the original on May 15, 2016.
^Girum T, Wasie A (December 2018). "Return of fertility after discontinuation of contraception: a systematic review and meta-analysis". Contraception and Reproductive Medicine. 3 (1): 9. doi:10.1186/s40834-018-0064-y. PMC 6055351. PMID 30062044.
^"Access to Contraception - ACOG". www.acog.org.
^"Who's Impacted by Attacks on Birth Control". www.plannedparenthoodaction.org. Retrieved October 15, 2019.
^Brown SS, Eisenberg L, et al. (Institute of Medicine (US) Committee on Unintended Pregnancy) (1995). Socioeconomic and Cultural Influences on Contraceptive Use. National Academies Press (US).
^"Just the Facts: Latinas & Contraception" (PDF). Archived from the original (PDF) on September 26, 2020. Retrieved March 25, 2020.
^Dehlendorf C, Rodriguez MI, Levy K, Borrero S, Steinauer J (March 2010). "Disparities in family planning". American Journal of Obstetrics and Gynecology. 202 (3): 214–20. doi:10.1016/j.ajog.2009.08.022. PMC 2835625. PMID 20207237.
^"Where can I get contraception?". NHS. December 21, 2017. Retrieved June 7, 2022.
^"Your contraception guide". NHS. December 21, 2017. Retrieved June 7, 2022.
^Willsher K (September 9, 2021). "France to offer free contraception to women under 25". The Guardian. Paris. Retrieved June 7, 2022.
^Conneely A (October 12, 2021). "Free contraception for women aged 17–25 from August". RTÉ. Retrieved June 7, 2022.
^"Minister Donnelly secures free contraception for women aged between 17–25 years in Budget 2022". Gov.ie. Department of Health. October 22, 2021. Retrieved June 7, 2022.
^ a b cSwan LE (December 2021). "The impact of US policy on contraceptive access: a policy analysis". Reproductive Health. 18 (1): 235. doi:10.1186/s12978-021-01289-3. ISSN 1742-4755. PMC 8607408. PMID 34809673.
^Sonfield A, Gold RB, Frost JJ, Darroch JE (March 2004). "U.S. Insurance Coverage of Contraceptives and the Impact Of Contraceptive Coverage Mandates". Perspectives on Sexual and Reproductive Health. 36 (2): 72–79. doi:10.1363/3607204. ISSN 1538-6341.
^"#FreeThePill Youth Council". Advocates for Youth. Retrieved June 7, 2022.
^Over-the-counter birth control? Drugmaker seeks FDA approval, AP News July 11, 2022
^Ibis celebrates the first-ever application for an OTC birth control pill in the United States, Ibis Reproductive Health July 2022
^Belluck P (July 13, 2023). "F.D.A. Approves First U.S. Over-the-Counter Birth Control Pill". The New York Times. ISSN 0362-4331. Retrieved July 13, 2023.
^ a b cJensen JT (October 2011). "The future of contraception: innovations in contraceptive agents: tomorrow's hormonal contraceptive agents and their clinical implications". American Journal of Obstetrics and Gynecology. 205 (4 Suppl): S21-5. doi:10.1016/j.ajog.2011.06.055. PMID 21961821.
^Halpern V, Raymond EG, Lopez LM (September 2014). "Repeated use of pre- and postcoital hormonal contraception for prevention of pregnancy". The Cochrane Database of Systematic Reviews. 2014 (9): CD007595. doi:10.1002/14651858.CD007595.pub3. PMC 7196890. PMID 25259677.
^ a bCastaño PM, Adekunle L (March 2010). "Transcervical sterilization". Seminars in Reproductive Medicine. 28 (2): 103–9. doi:10.1055/s-0030-1248134. PMID 20352559. S2CID 260317985.
^Rabin RC (November 21, 2016). "Bayer's Essure Contraceptive Implant, Now With a Warning". The New York Times. ISSN 0362-4331. Retrieved May 1, 2020.
^Office of the Commissioner (March 24, 2020). "FDA takes additional action to better understand safety of Essure, inform patients of potential risks". FDA. Retrieved May 1, 2020.
^Kaplan S (July 20, 2018). "Bayer Will Stop Selling the Troubled Essure Birth Control Implants". The New York Times. ISSN 0362-4331. Retrieved May 1, 2020.
^Friedman M (2019). "Interest Among U.S. Men for New Male Contraceptive Options" (PDF). Male Contraceptive Initiative. Retrieved October 12, 2023.
^Glasier A (November 2010). "Acceptability of contraception for men: a review". Contraception. 82 (5): 453–456. doi:10.1016/j.contraception.2010.03.016. PMID 20933119.
^Roth MY, Shih G, Ilani N, Wang C, Page ST, Bremner WJ, et al. (October 2014). "Acceptability of a transdermal gel-based male hormonal contraceptive in a randomized controlled trial". Contraception. 90 (4): 407–412. doi:10.1016/j.contraception.2014.05.013. PMC 4269220. PMID 24981149.
^Wang CC. "Male Birth Control Is in Development, but Barriers Still Stand in the Way". Scientific American. Retrieved October 12, 2023.
^"Birth control for men". Chemical & Engineering News. Retrieved October 12, 2023.
^Sitruk-Ware R (May 11, 2018). "Getting contraceptives for men to the market will take pharma's help". STAT. Retrieved October 12, 2023.
^"G-FINDER data portal". Policy Cures Research. Retrieved October 12, 2023.
^"CDP Research: Developing Hormonal Contraception Methods for Men | NICHD – Eunice Kennedy Shriver National Institute of Child Health and Human Development". www.nichd.nih.gov. February 16, 2022. Retrieved October 12, 2023.
^Gorvett Z. "The weird reasons there still isn't a male contraceptive pill". BBC Future.
^Gibbens S (March 3, 2023). "Birth control options for men are advancing. Here's how they work". National Geographic Magazine. Archived from the original on March 3, 2023. Retrieved October 12, 2023.
^Barber R (December 4, 2022). "In the hunt for a male contraceptive, scientists look to stop sperm in their tracks". National Public Radio. Retrieved October 12, 2023.
^Chiu A (April 14, 2022). "Why there's still no new birth control for men". Washington Post. Retrieved October 12, 2023.
^Blum D (March 25, 2022). "Despite Encouraging Research, a Male Birth Control Pill Remains Elusive". The New York Times. ISSN 0362-4331. Retrieved October 12, 2023.
^"What Is In Development". Male Contraceptive Initiative. Retrieved October 12, 2023.
^Anderson DJ, Johnston DS (April 2023). "A brief history and future prospects of contraception". Science. 380 (6641): 154–158. Bibcode:2023Sci...380..154A. doi:10.1126/science.adf9341. PMC 10615352. PMID 37053322. S2CID 258112296.
^Abbe CR, Page ST, Thirumalai A (September 2020). "Male Contraception". The Yale Journal of Biology and Medicine. 93 (4): 603–613. PMC 7513428. PMID 33005125.
^Holdaway J, Georg GI (May 24, 2024). "An emerging target for male contraception". Science. 384 (6698): 849–850. Bibcode:2024Sci...384..849H. doi:10.1126/science.adp6432. ISSN 0036-8075. PMID 38781397.
^Millar L (2011). Infectious Disease Management in Animal Shelters. John Wiley & Sons. ISBN 978-1-119-94945-9. Archived from the original on May 3, 2016.
^Ackerman L, ed. (2007). Blackwell's five-minute veterinary practice management consult (1st ed.). Ames, IO: Blackwell Pub. p. 80. ISBN 978-0-7817-5984-7. Archived from the original on June 10, 2016.
^Boyle R (March 3, 2009). "Birth control for animals: a scientific approach to limiting the wildlife population explosion". Popular Science. New York: PopSci.com. Archived from the original on May 25, 2012.
^Kirkpatrick JF, Lyda RO, Frank KM (July 2011). "Contraceptive vaccines for wildlife: a review". American Journal of Reproductive Immunology. 66 (1): 40–50. doi:10.1111/j.1600-0897.2011.01003.x. PMID 21501279. S2CID 3890080.
^Levy JK (July 2011). "Contraceptive vaccines for the humane control of community cat populations". American Journal of Reproductive Immunology. 66 (1): 63–70. doi:10.1111/j.1600-0897.2011.01005.x. PMC 5567843. PMID 21501281.
^"Goat 'condoms' save Kenyan herds". BBC News. October 6, 2008. Archived from the original on October 6, 2008. Retrieved October 6, 2008.
Further reading
Speroff L, Darney PD (2010). A clinical guide for contraception (5th ed.). Philadelphia: Lippincott Williams & Wilkins. pp. 242–43. ISBN 978-1-60831-610-6. Archived from the original on May 6, 2016.
Stubblefield PG, Roncari DM (2011). "Family Planning". In Berek JS (ed.). Berek & Novak's Gynecology (15th ed.). Philadelphia: Lippincott Williams & Wilkins. pp. 211–69. ISBN 978-1-4511-1433-1.
Jensen JT, Mishell Jr DR (March 2012). "Family Planning: Contraception, Sterilization, and Pregnancy Termination". In Lentz GM, Lobo RA, Gershenson DM, Katz VL (eds.). Comprehensive Gynecology (6th ed.). Philadelphia: Mosby Elsevier. pp. 215–72. ISBN 978-0-323-06986-1.
Gavin L, Moskosky S, Carter M, Curtis K, Glass E, Godfrey E, et al. (Division of Reproductive Health, National Center for Chronic Disease Prevention and Health Promotion, CDC) (April 2014). "Providing quality family planning services: Recommendations of CDC and the U.S. Office of Population Affairs". MMWR. Recommendations and Reports. 63 (RR-04): 1–54. PMID 24759690.
World Health Organization Department of Reproductive Health and Research and Johns Hopkins Bloomberg School of Public Health (2011). Family planning: A global handbook for providers: Evidence-based guidance developed through worldwide collaboration (PDF) (Rev. and Updated ed.). Geneva: WHO and Center for Communication Programs. ISBN 978-0-9788563-7-3.
Curtis KM, Jatlaoui TC, Tepper NK, Zapata LB, Horton LG, Jamieson DJ, Whiteman MK (July 2016). "U.S. Selected Practice Recommendations for Contraceptive Use, 2016". MMWR. Recommendations and Reports. 65 (4): 1–66. doi:10.15585/mmwr.rr6504a1. PMID 27467319.



.jpg/1280px-Geburtenkontrollkette_(cropped).jpg)
.jpg/1280px-Emergency_contraceptive_(cropped).jpg)



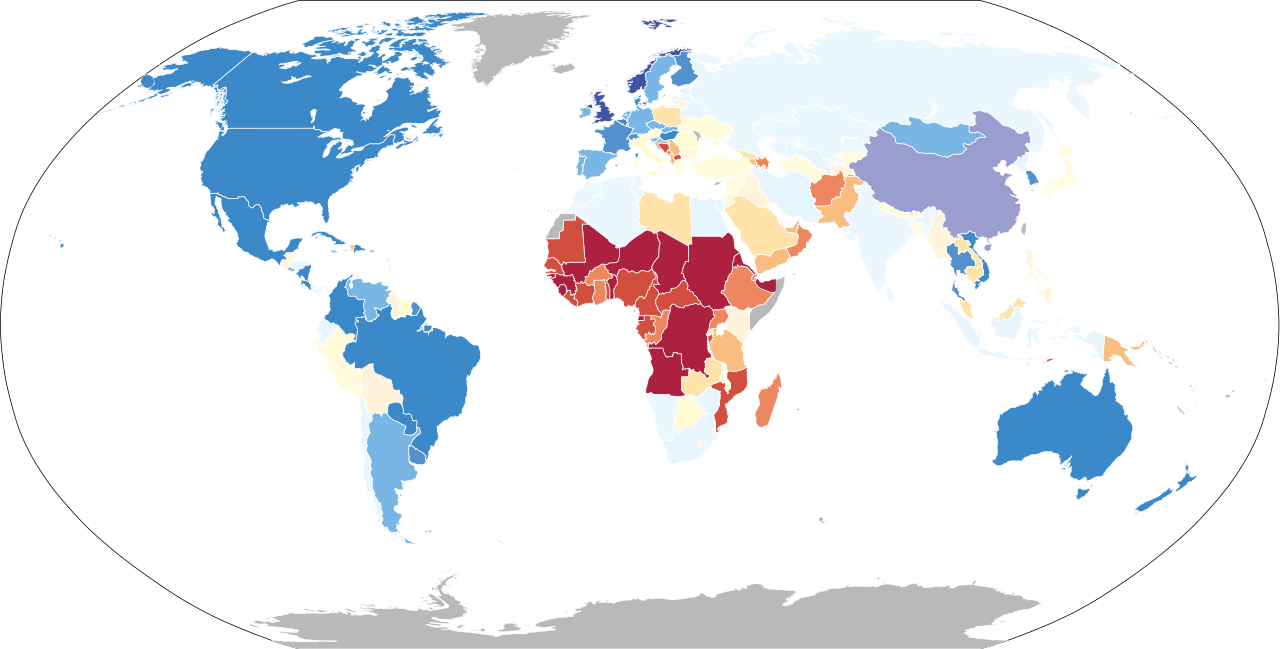








{kind=link}